You roll over in bed in Quincy, sit up, and the room seems to spin. Or you’re walking near the water in Plymouth and suddenly feel off balance, like your body isn’t quite catching up with where your head is. For a lot of South Shore residents, that moment is more than unsettling. It’s disruptive, frustrating, and sometimes scary.
It also raises a basic question fast. What causes dizziness and vertigo? Those terms often get used together, but they don’t always mean the same thing. Dizziness is a broad word people use for lightheadedness, floating, unsteadiness, or feeling “off.” Vertigo is more specific. It’s the false sense that you or the room is moving or spinning.
That distinction matters because the cause matters. Some cases come from the inner ear. Others are tied to migraine, medication side effects, blood pressure changes, or another health issue entirely. The good news is that many of the dizziness and vertigo problems we see across the South Shore are treatable, especially when someone gets the right evaluation instead of guessing.
At local clinics from Quincy to Hanover to Plymouth, one of the most helpful things we do is sort out what pattern your symptoms fit. People often come in saying, “I’m dizzy,” but the specific answer starts showing up in the details. Did it happen when you looked up? Rolled in bed? Stood up too quickly? Start after a virus? Come with headache, light sensitivity, or nausea? Those clues point us in very different directions.
Table of Contents
- Feeling Unsteady on the South Shore? An Introduction to Dizziness and Vertigo
- The Most Common Vertigo Causes We Treat in Our South Shore Clinics
- Could It Be Something Else? Other Potential Causes of Dizziness
- What to Expect at Your First Dizziness and Vertigo PT Appointment
- How Vestibular Therapy Helps You Reclaim Your Balance
- Red Flag Symptoms When to Seek Emergency Care
- Stop Spinning and Start Living Find Dizziness Relief Near You
Feeling Unsteady on the South Shore? An Introduction to Dizziness and Vertigo
You get out of bed in Quincy, turn to shut off the alarm, and the room seems to shift. Or you are walking the aisles at the grocery store in Hanover and feel off balance for no clear reason. By the time symptoms hit during a commute, a workout, or a trip down the stairs at home in Plymouth, many people are already wondering the same thing. Is this vertigo, dizziness, or something more serious?
We hear that question every week in our South Shore clinics. Dizziness is common, especially as people get older, but the label alone does not tell you what is wrong. The pattern matters. What you feel, what brings it on, how long it lasts, and whether it shows up with head motion, standing, walking, or visual motion all point us in different directions.
Dizziness and vertigo are not the same symptom
Patients use the word "dizzy" to describe several very different problems. Sorting that out is one of the first things we do at Peak, because the right treatment depends on the exact sensation.
| Symptom feeling | What patients often mean |
|---|---|
| Lightheaded | “I feel faint” or “I get a head rush” |
| Off balance | “I drift when I walk” or “I feel shaky” |
| Floating or foggy | “I don’t feel grounded” |
| Spinning | “The room moves when I turn over” |
Spinning vertigo often points toward the inner ear. Lightheadedness after standing can fit a blood pressure issue. A foggy, unsettled feeling after a blow to the head may call for concussion management and vestibular rehabilitation. The words patients choose give us useful clues, but the movement history usually gives us even more.
A simple example. If symptoms show up when you roll in bed, tip your head back, or bend to pick something up, I start thinking about positional vertigo. If symptoms happen in busy stores, while walking, or after quick head turns, I start looking at how the vestibular system, eyes, and balance centers are working together.
Why local evaluation matters
People on the South Shore do not need another vague answer to "why am I dizzy?" They need a plan that fits daily life here. That means being able to drive without gripping the wheel, shop without veering, get through work without that washed-out feeling, and turn over in bed without bracing for another spin.
In clinic, the goal is not just to name the symptom. The goal is to identify the source and match it to the right next step. Sometimes that means a repositioning maneuver in the first visit. Sometimes it means balance testing, gaze stabilization work, or coordination with your physician if the pattern does not fit a vestibular problem.
That practical difference matters in towns like Quincy, Hanover, and Plymouth, where people want to get back to work, family routines, and being active without feeling uncertain every time they move their head.
The Most Common Vertigo Causes We Treat in Our South Shore Clinics
A lot of South Shore patients come in worried that vertigo must mean something rare or dangerous. In practice, the patterns are usually familiar. The key is matching the symptom story to the right exam, because the treatment for brief bed-turning vertigo is very different from the treatment for dizziness that started after an illness or head injury.
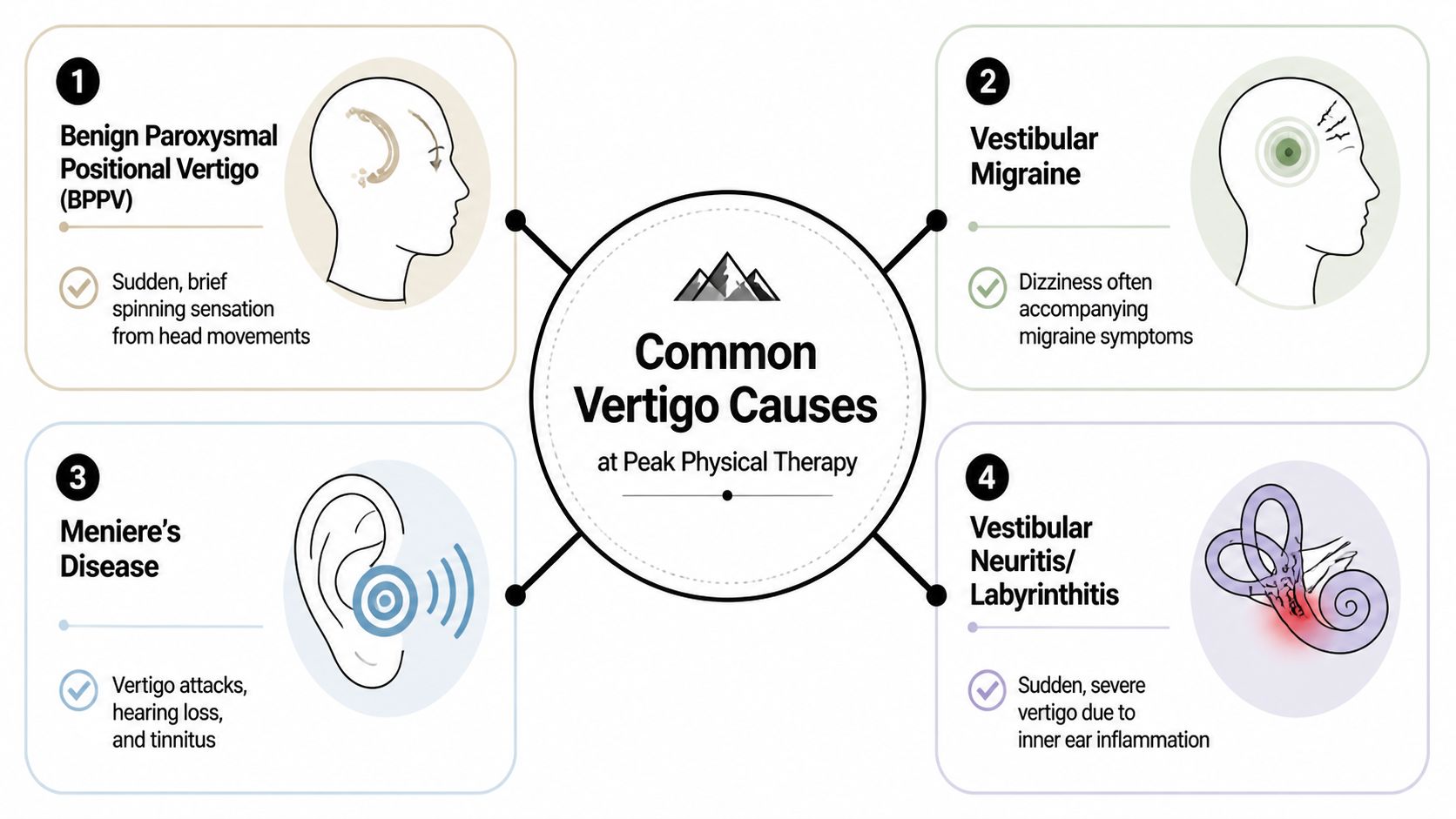
BPPV and the loose crystal problem
The most common vertigo diagnosis we treat in clinic is benign paroxysmal positional vertigo, or BPPV. It happens when small calcium crystals shift into the wrong part of the inner ear and start sending the brain bad motion signals. Patients in Quincy, Hanover, and Plymouth often describe the same pattern. Rolling in bed, looking up into a cabinet, or bending down to tie a shoe brings on a short, intense spin.
BPPV usually responds well to the right repositioning maneuver. That matters because people often spend weeks trying to avoid movement when the better option is a targeted mechanical treatment. In clinic, we test the specific canal involved and choose the maneuver that fits, instead of handing out generic advice and hoping it settles down on its own.
Vestibular neuritis after illness
Another common cause is vestibular neuritis. This pattern looks very different from BPPV. Instead of a few seconds of spinning with a position change, the dizziness is often stronger, lasts longer, and can show up after a virus or other illness.
Patients often say they woke up and could barely walk straight. Nausea is common. Head movement feels awful. Once the worst phase passes, the problem often shifts from acute spinning to lingering imbalance, motion sensitivity, and fatigue in busy environments. That is where vestibular therapy helps. We use graded movement, gaze stabilization, and balance retraining to help the brain recalibrate.
Rest may help early. Too much rest later tends to slow progress.
Vestibular migraine and visually triggered dizziness
Vestibular migraine is another diagnosis we see often, and it can be easy to miss because the person is not always dealing with a classic headache during the dizzy spell. The symptom picture may include motion sensitivity, visual overwhelm, light or noise sensitivity, fogginess, and episodes that flare with sleep changes, stress, screens, or crowded stores.
In a South Shore clinic, this matters for a simple reason. Someone can feel fine sitting still at home but get wiped out walking through a supermarket in Weymouth or turning quickly in a busy workplace. Treatment is different from BPPV. We look at visual-vestibular tolerance, head movement tolerance, balance, and triggers, then build a plan that settles the system without overloading it.
If symptoms began after a blow to the head, or the dizziness comes with headache, light sensitivity, and balance trouble, we may also coordinate care through concussion management and vestibular rehabilitation at Peak.
When hearing symptoms change the picture
Vertigo with ringing, ear fullness, or hearing changes raises different questions. In those cases, conditions such as Meniere’s disease or other inner-ear problems move higher on the list. Physical therapy can still help with balance and motion sensitivity, but hearing symptoms often mean the exam should include medical follow-up with an ENT or physician.
That trade-off is important. Some dizziness problems respond well to treatment in the PT clinic right away. Some need co-management so the patient gets the right diagnosis and does not waste time on the wrong plan.
A smaller group of patients also describes dizziness that sounds less like vertigo and more like lightheadedness, heart racing, or feeling faint when upright. If that pattern sounds familiar, this overview of root-cause strategies for POTS may be a useful starting point while we sort out whether the issue fits a vestibular problem or something else entirely.
Could It Be Something Else? Other Potential Causes of Dizziness
Not all dizziness is vertigo, and not all dizziness comes from the inner ear. That’s where people often get stuck. They assume every dizzy spell must be “crystals,” when sometimes the actual cause sits somewhere else entirely.

Blood pressure and positional dizziness
One common non-vertigo complaint is the quick wave of dizziness that happens when you stand up. Patients call it a head rush. It usually feels different from room-spinning vertigo. Instead of motion, it’s more like a sudden drop in steadiness or a brief dimming out.
That pattern can point toward blood pressure regulation rather than an inner ear issue. We look at timing, symptom behavior, and what position changes bring it on. If someone says, “I’m fine in bed, fine turning my head, but standing from a chair gets me every time,” that tells us to widen the lens.
Some patients with positional symptoms also ask about autonomic issues. If that conversation applies to your case, this overview of root-cause strategies for POTS gives a useful starting point for understanding one broader category of blood flow and heart-rate regulation problems.
Medication side effects in older adults
For many older adults, medication is the missing piece. This gets overlooked all the time. A person starts a new prescription, changes a dose, or adds another medication, then weeks later starts feeling unsteady and assumes it’s just aging.
That assumption can be a mistake. The practical concern for South Shore families is simple. Medication side effects are a major, often overlooked cause of dizziness, especially when someone takes multiple prescriptions, as described in this Henry Ford article on possible causes of dizziness. In clinic, one of the most useful things we can do is help patients notice whether the timing of their symptoms matches medication changes so they can have a more informed conversation with their doctor.
Here’s when medication deserves extra attention:
- Symptoms started after a medication change and there wasn’t a clear illness or positional trigger.
- The dizziness feels general, not clearly spinning.
- You feel more unsteady at certain times of day, such as shortly after taking pills.
- You’re taking several medications at once and can’t tell which change mattered.
Many people blame dizziness on “getting older” when the better question is, “What changed?”
Anxiety, sensory overload, and persistent unsteadiness
Anxiety doesn’t make dizziness imaginary. It can change breathing patterns, body tension, motion sensitivity, and how the nervous system interprets movement. Some people feel worse in crowded stores, on escalators, in bright environments, or when they haven’t felt steady for a while and start anticipating the next episode.
This is also why migraine-related dizziness can blur into visual overload and neck tension. If that sounds familiar, this article on physical therapy and migraines can help connect some of those patterns.
The key trade-off is this. If you assume anxiety is the only cause, you can miss an ear or migraine issue. If you ignore the nervous system side completely, recovery can drag out because the brain stays on high alert. Good care looks at both.
What to Expect at Your First Dizziness and Vertigo PT Appointment
You wake up in Quincy, sit up in bed, and the room spins hard enough that you grab the mattress and wait it out. By the time you get to your appointment, a lot of people are worried we’re going to make that happen over and over. A good first visit is more controlled than that. The goal is to find the pattern quickly, test what matters, and keep the exam tolerable.

In our South Shore clinics, the first appointment usually starts with listening. The details matter more than people expect. A brief spinning spell when you roll to one side points us in a very different direction than hours of fogginess in a grocery store or a washed-out feeling when you stand up too fast.
The conversation comes first
We start by getting specific about the symptom, because “dizzy” can mean several different problems.
We’ll ask:
- What does it feel like? Spinning, rocking, floating, lightheaded, off-balance, or visually overwhelmed?
- What brings it on? Rolling in bed, looking up, quick turns, busy stores, screens, walking outside, standing up?
- How long does it last? Seconds, minutes, hours, or most of the day?
- What comes with it? Nausea, headache, hearing changes, ear pressure, neck pain, recent illness, or falls?
This part guides the whole visit. If the story sounds like a crystal problem, we test for that. If it sounds more like motion sensitivity, migraine, or a balance system that has gotten less reliable, we shift the exam in that direction.
The exam is targeted
After the history, we look at how your eyes, inner ear, head motion, and balance systems are working together. That can include positional testing, eye movement testing, walking and standing balance, and checking how well you tolerate head turns or visual motion.
Here’s the practical trade-off. Some tests may briefly bring on symptoms, but avoiding all symptom provocation can leave you with a vague answer and the wrong plan. We use only the testing needed to identify the pattern, then stop. In clinic, that often means a short symptom flare that gives us a much clearer path to treatment.
| What we test | What it can reveal |
|---|---|
| Positional testing | Whether specific head movements trigger vertigo in a repeatable way |
| Eye movement response | Whether the vestibular system is sending the wrong signal |
| Balance in standing and walking | How much your stability and fall risk have changed |
| Visual motion tolerance | Whether stores, traffic, or screen-heavy environments are driving symptoms |
A good vestibular exam is organized. It does not chase every possibility at once.
What you’ll leave with
By the end of the first visit, you should know what pattern your symptoms fit and what the next step is. For some South Shore patients, that means a repositioning maneuver the same day. For others, it means starting vestibular rehab, building a home plan, and setting expectations for how recovery usually feels week to week.
You should also leave with a plan that makes daily life easier right away. That may include advice on bed mobility, walking safety, driving, screen use, or a few simple home activities to keep your balance system active between visits. If general strengthening is part of the picture, we may also point you to balance exercises for older adults that support steadier walking and safer movement at home.
Sometimes the right outcome of the first visit is a referral back to your physician. That is good care, not a dead end. If your symptoms fit medication side effects, migraine, blood pressure changes, or another medical issue, we’ll tell you that clearly so you know what to do next. At Peak clinics in places like Quincy, Hanover, and Plymouth, that local access means you can get answers close to home and start the right care without guessing.
How Vestibular Therapy Helps You Reclaim Your Balance
Good vestibular therapy should make daily life feel more manageable, not more confusing. Once the cause of dizziness is clear, treatment becomes specific. We match the plan to the problem, whether that means repositioning loose crystals, improving eye-head coordination, reducing motion sensitivity, or rebuilding balance after weeks of feeling unsteady.

Vestibular symptoms also overlap with other conditions, including migraine and general balance decline. That is part of why persistent dizziness deserves a careful plan instead of guesswork. In clinic, we look at what triggers symptoms, what calms them down, and how they affect walking, driving, shopping, work, and sleep.
For BPPV, precision matters
If BPPV is causing the spinning, the fastest treatment is often a canalith repositioning maneuver done in the right direction for the affected canal. General balance work will not move those displaced crystals back where they belong.
That detail matters more than people expect. I often meet South Shore patients who have tried rest, searched for exercises online, or avoided turning in bed for weeks because every roll sets the room spinning. A correctly chosen maneuver is usually a much better use of time.
After treatment, patients commonly notice one of a few patterns:
- Fast relief, especially when the diagnosis is clear
- A mildly off or heavy-headed feeling for a short time afterward
- Partial improvement, with a repeat maneuver or follow-up visit needed
All three can be normal. The goal is not to chase a perfect feeling in the first hour. The goal is to get the right system moving in the right direction.
For lingering dizziness, retraining works better than avoiding movement
Some dizziness hangs around after a virus, a migraine flare, a concussion, or a stretch of symptoms that taught the body to brace against movement. In those cases, the inner ear and brain are often sending mixed signals. Physical therapy helps them work together again through repeated, graded practice.
Treatment may include:
- Gaze stabilization so your eyes stay focused while your head moves
- Habituation exercises to reduce symptoms with positions or environments that set you off
- Balance training to improve steadiness on firm ground, uneven ground, and during changes in direction
- Walking and turning drills that bring the work back to real life
Around the South Shore, that may mean walking uneven sidewalks in Quincy with more confidence, getting through a grocery store in Hanover without feeling overloaded, or turning quickly in the kitchen in Plymouth without needing to stop and brace.
Home work matters too, but it should fit the reason you are dizzy. If you want a few safe ideas for general steadiness, these balance exercises for older adults at home can be a helpful starting point. They do not replace a vestibular evaluation when dizziness is the main problem.
What usually helps, and what tends to slow recovery
The trade-off in vestibular rehab is simple. Rest can make you feel safer in the short term, but too much avoidance often keeps the system sensitive. Pushing too hard can flare symptoms. The right plan sits in the middle. It challenges your balance enough to drive recovery without overwhelming you.
What tends to help:
- A clear diagnosis tied to your actual symptoms
- Exercises chosen for your vestibular problem, not random dizziness advice
- Gradual return to head movement, walking, and normal routines
- Real-time adjustments based on how your body responds
What tends to slow progress:
- Avoiding movement for too long
- Doing the same generic exercise plan for every dizzy spell
- Stopping activity completely after symptoms start
- Trying to self-treat without knowing the cause
At Peak Physical Therapy and Sports Performance, that clinic-based approach gives patients something home guessing cannot. In Quincy, Hanover, Plymouth, and other South Shore communities, you can have a therapist watch your eye movements, balance, and symptom response in real time, then adjust the plan so treatment matches what your body is doing.
Red Flag Symptoms When to Seek Emergency Care
Most dizziness is not an emergency, but some symptoms change the picture completely. If dizziness or vertigo shows up with signs that suggest a possible stroke or other acute neurological event, don’t wait for a PT appointment.
Seek emergency care right away, call 911, or go to the nearest emergency room if dizziness comes with any of the following:
- Sudden weakness or numbness on one side of the face, arm, or leg
- Trouble speaking or understanding speech
- Double vision or sudden vision loss
- A sudden severe headache that feels unusual or extreme
- Loss of coordination that is new and dramatic
- Chest pain, fainting, or severe shortness of breath
- New confusion or difficulty staying awake
- A fall with head injury, especially if symptoms worsen afterward
When not to wait it out
The hardest part for many people is knowing whether they’re overreacting. In this situation, it’s safer to act. If symptoms are abrupt, intense, and clearly different from anything you’ve felt before, emergency evaluation comes first.
If dizziness is paired with stroke-like symptoms, the right first step is emergency medical care, not outpatient rehab.
A responsible dizziness workup always includes knowing when physical therapy is appropriate and when it isn’t. If a medical emergency is possible, that has to be ruled out before anything else.
Stop Spinning and Start Living Find Dizziness Relief Near You
A lot of people on the South Shore wait longer than they need to.
They stop rolling onto one side in bed. They hold the cart a little tighter at the grocery store in Quincy. They avoid quick head turns while driving through Hanover or walking the waterfront in Plymouth. After a few weeks, life gets smaller, and confidence usually drops with it.
The good news is that dizziness often responds well to the right kind of evaluation and treatment. The key is figuring out which system is driving the problem. In clinic, I look at the pattern carefully. Does the room spin with position changes? Do busy spaces trigger symptoms? Is balance worse in the dark, after an illness, or after starting a new medication? Those details help sort out whether physical therapy is likely to help, whether another provider should be involved, or both.
Local care makes that process easier. If you live in Braintree, Quincy, Weymouth, Cohasset, Duxbury, East Bridgewater, Hanover, Kingston, Milton, Norwell, Pembroke, Plymouth, or Scituate, you can get answers close to home from a team that treats dizziness regularly and knows how much these symptoms affect day-to-day life.
You do not need to wait until you fall.
If rolling in bed makes the room spin, aisles and crowds leave you foggy, quick turns throw you off, or you have started second-guessing your balance on stairs, that is reason enough to get checked. At Peak, patients can expect a focused exam, plain-English explanations, and a treatment plan built around what is triggering symptoms, not a generic handout.
If dizziness or vertigo is affecting your day, book an appointment with Peak Physical Therapy and Sports Performance. With South Shore clinics in Braintree, Quincy, Weymouth, Cohasset, Duxbury, East Bridgewater, Hanover, Kingston, Milton, Norwell, Pembroke, Plymouth, and Scituate, you can get a local evaluation, a clear plan, and practical treatment close to home.