A lot of people notice hip flexor pain when walking in the most ordinary moments. Not during a sprint. Not in the middle of a hard workout. It shows up when you step off the curb, climb out of the car, head into work, or try to enjoy a simple walk without thinking about your body.
That can feel surprisingly discouraging. When pain starts in the front of the hip or groin with every few steps, it is easy to wonder whether you should push through it, rest completely, or worry that something more serious is going on.
On the South Shore, we see this pattern often. A commuter has spent months sitting more than usual through winter. A recreational runner starts back up in spring. A parent joins weekend walks, golf, hiking, or pickup sports and suddenly the front of the hip feels sharp, tight, or “stuck.” The problem is not always a dramatic injury. Often, it is a very treatable mismatch between what the tissue can handle and what you suddenly asked it to do.
That Nagging Pain in Your Hip When You Walk
You may feel it leaving the house for a walk near Scituate Harbor. Or stepping out at the T after a long commute. The first few steps feel stiff, then you lift your knee and get that familiar pinch in the front of the hip.

For some people, it is a nagging ache. For others, it is sharp enough to change the way they walk. You may catch yourself shortening your stride, leaning back, or avoiding stairs because lifting the leg feels worse than standing still.
Why this feels so frustrating
Hip flexor pain when walking disrupts everyday life fast. Walking is supposed to be automatic. When it hurts, even routine errands start to feel like a decision.
Common reactions we hear from patients include:
- Worry about damage: “Did I tear something?”
- Fear of making it worse: “Should I stop exercising completely?”
- Frustration with inconsistency: “It hurts after sitting, then eases a bit, then comes back.”
- A sense of lost momentum: “I was finally getting active again.”
That last one matters. In Massachusetts, this often shows up in seasonal waves. Winter routines get quieter. Sitting time goes up. Then warmer weather arrives and activity jumps before the hips are ready.
The good news
Most front-of-hip pain with walking is not random. It usually follows a pattern. Once you identify whether the main driver is strain, tightness, weakness, gait compensation, or irritation from a sudden activity increase, treatment becomes much clearer.
Key takeaway: Pain at the front of the hip during walking is common, understandable, and usually responsive to the right combination of load management, mobility work, and progressive strengthening.
You do not need to guess your way through it. A careful physical therapy evaluation can sort out what is irritated, what is weak, and what movement habit keeps reloading the same spot.
Why Your Hip Flexors Hurt During a Simple Walk
Your hip flexors are the muscles that help lift your thigh and bring your leg forward. The two most important ones in this conversation are the iliopsoas and the rectus femoris.
Think of them like strong guide wires at the front of the hip. They help move the leg, but they also help control the position of the pelvis as you move from one step to the next. If they are strained, tight, or overloaded, walking stops feeling simple.
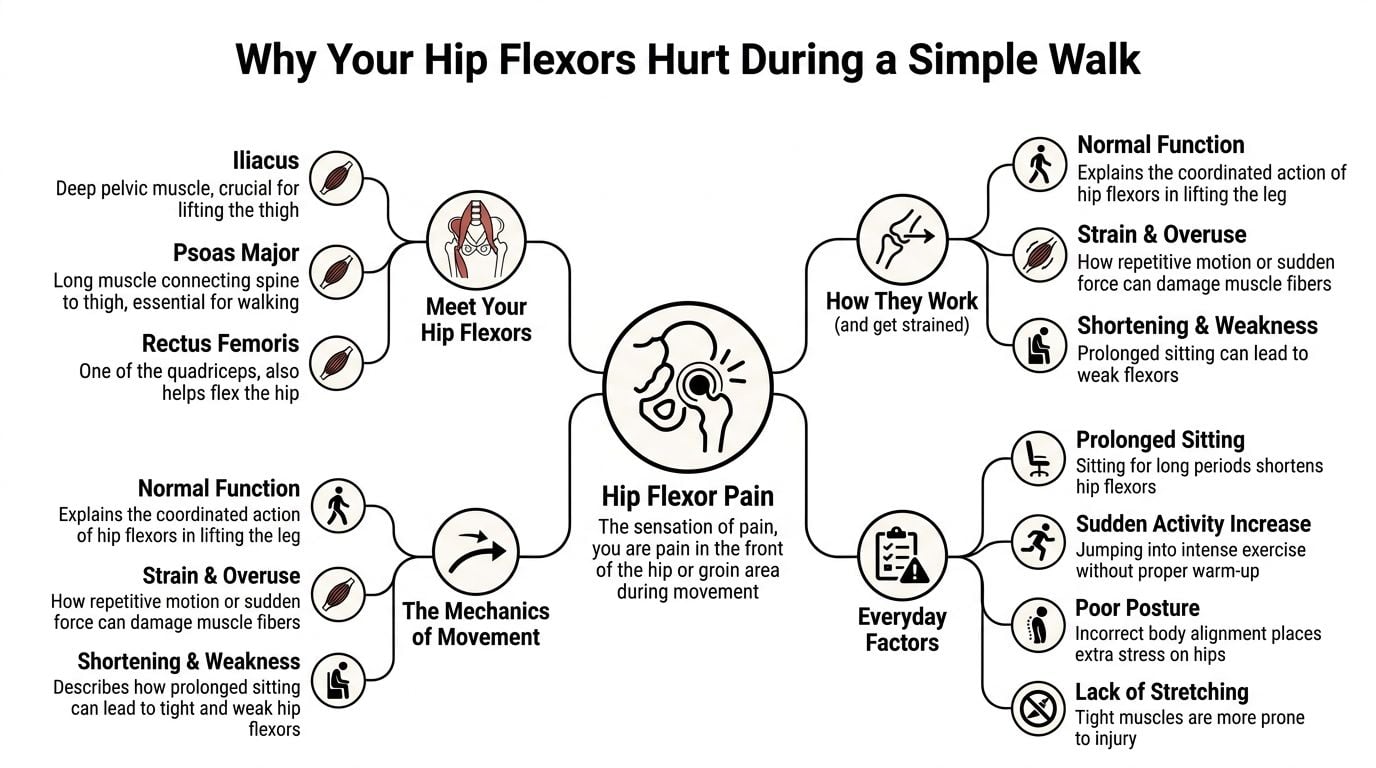
What these muscles do
The iliopsoas is the primary hip flexor. It starts deep in the front of the pelvis and lower spine and attaches to the top of the thigh bone. The rectus femoris crosses both the hip and knee, so it helps with hip flexion and knee extension.
When those muscles are healthy, they help you:
- Lift the leg forward during walking
- Climb stairs and step uphill
- Rise from sitting
- Control pelvic position so you do not compensate through the low back
When they are irritated, those same motions can create pain at the front of the hip.
Why walking hurts more than people expect
Walking seems gentle, but the hip flexors work hard during the swing phase, when your leg leaves the ground and moves forward. During that part of gait, your hip flexors generate 40 to 60% of their maximum voluntary contraction, and peak iliopsoas activation occurs at 20 to 30% of the gait cycle. That is one reason pain often spikes just as you start lifting the leg forward during a step (Alexander Orthopaedics).
If the tissue is strained, even mildly, every step repeats the same load. That creates a simple but stubborn cycle: lift the leg, stress the irritated fibers, feel pain, compensate, then stress nearby areas too.
The deconditioning and load spike problem
This is the part many generic articles miss.
A lot of Massachusetts residents are not dealing with pure sports overuse. They are dealing with deconditioning plus a sudden jump in activity. Months of sitting shorten the front of the hip and reduce tolerance for load. Then spring running starts. Golf season starts. Walking routes get longer. Weekend hiking returns.
That combination often creates hip flexor pain when walking because the muscle is both tight and underprepared.
A few practical contributors show up again and again:
- Prolonged sitting: The hip stays in a flexed position for hours.
- Sudden return to exercise: The tissue has not rebuilt capacity yet.
- Poor stride mechanics: Short, guarded steps can keep the front of the hip irritated.
- Footwear mismatch: If you spend long days on your feet at work, shoe support matters. For readers also dealing with fatigue from standing, this guide to boots for standing all day can be a useful starting point when thinking about lower-body load from the ground up.
PT perspective: Rest alone can calm a flare, but it does not rebuild the strength and control your hip flexors need for repeated walking.
What works better than random stretching
Aggressive stretching usually is not the whole answer. If the tissue is actively irritated, pulling harder on it can make it angrier. What tends to work better is a sequence: reduce irritation, restore mobility where needed, strengthen the hip flexors and surrounding muscles, then retrain walking mechanics.
That is how you get from “every step reminds me of it” to walking normally again.
Common Causes of Hip Flexor Pain for Massachusetts Residents
Hip flexor pain when walking is not one-size-fits-all. The front of the hip can hurt for similar reasons in different people, but the daily habits driving it are often very specific.

The desk-bound commuter
This is one of the most common South Shore patterns. Long drives, long desk hours, and too few movement breaks leave the front of the hip in a shortened position day after day.
A 2023 study found hip flexor tightness in 94.3% of young adults, with a strong link to sedentary behavior (IJFMR study). Clinically, that matters because a tight hip flexor can pull the pelvis forward and increase strain through both the front of the hip and the low back.
Typical signs include:
- Pain after sitting: The first steps feel stiff or pinchy
- Discomfort with stairs or hills: Lifting the knee is more provocative
- Low back tightness: The pelvis tips forward and the back picks up extra work
This is why “I only walk for exercise” does not always protect you. If your baseline is mostly sitting, even normal walking volume can feel like a big load increase.
The seasonal athlete
This is the deconditioning plus load spike group. It is common after winter in Massachusetts.
Someone goes from lower activity to spring road races, long walks, softball, golf, or weekend hiking. The tissue has not adapted yet, but motivation is high. The hip flexor ends up absorbing more load than it can currently manage.
What usually does not work:
- Doing nothing all week, then being very active on weekends
- Pushing through front-of-hip pain because “it’s just tight”
- Adding a lot of stretching but no strength work
- Returning to hills, speed work, or long walks too soon
What works better is a gradual ramp in capacity. That means spacing activity, adding strength, and respecting early warning signs instead of waiting for a sharper strain.
If your symptoms are part of a larger hip issue, our guide to hip pain and thigh pain can help you understand related patterns.
The dedicated athlete
Teens and young adults in sports like soccer and hockey are another group we watch closely. In collegiate athletes across 25 NCAA sports, hip flexor strains occurred at a rate of 1.60 per 10,000 athlete-exposures, with 770 total cases reported. The study also found higher rates in men’s soccer and ice hockey, and 59.4% of injuries occurred through noncontact mechanisms such as sudden deceleration or kicking (PubMed study).
That matters locally because South Shore athletes often layer school sports, club seasons, strength training, and showcases with very little true recovery. A player from Hingham, Duxbury, or Quincy may not remember one dramatic event. Instead, the front of the hip gradually becomes sore, then painful with walking, cutting, or lifting the knee.
A few causes people overlook
Not every case starts with exercise.
Sometimes hip flexor pain when walking follows:
- A change in work demands
- A long period of inactivity after illness or another injury
- Compensation from knee, foot, or back pain
- Shoveling snow, then abruptly returning to spring activity
Local reality: We often see flare-ups when a sedentary winter is followed by a sudden burst of warmer-weather activity. The issue is not laziness or bad luck. It is a mismatch between tissue capacity and load.
The key is identifying which version of the problem you have. Tightness, weakness, gait compensation, and training errors can all create similar pain. The treatment needs to match the driver.
When to Worry Is It More Than a Simple Strain
A lot of front-of-hip pain with walking is muscular and responds well to the right plan. Still, some patterns deserve quicker attention, especially if your pain showed up after a sudden jump in activity following a low-activity winter.
That pattern is common here on the South Shore. A desk worker spends months sitting more, then spring arrives and they jump into running, long walks, yard work, or weekend hikes. The hip flexors are asked to handle more load than they are ready for. Sometimes that leads to a simple strain. Sometimes it exposes a different problem that should not be brushed off.
Signs that fit a common strain
A straightforward hip flexor strain often includes:
- Pain in the front of the hip or groin
- Discomfort when lifting the knee, walking faster, or climbing stairs
- Symptoms that ease with rest
- Localized soreness rather than broad pain
- A limp that improves as the irritation calms down
Education also plays a key role here. Mild pain does not always mean minor tissue damage, and sharp pain does not always mean something serious. What matters is the full pattern. If symptoms are tied to activity, stay fairly local, and begin settling within a short window, a muscle strain is more likely.
Red flags that need quicker evaluation
Get medical care promptly if you have:
- Inability to bear weight
- A sudden pop followed by severe pain
- Marked swelling or bruising
- Severe or persistent night pain
- Numbness, tingling, or pain that radiates
- Fever or feeling unwell along with hip pain
- Pain after a fall or direct blow
- Symptoms that keep getting worse despite rest
These signs raise concern for something other than an irritated hip flexor, such as a more significant muscle injury, a joint issue, a back-related problem, or, in some cases, a bone stress injury.
The practical decision
Here is the trade-off. Resting for a day or two can calm an irritated muscle. Resting for weeks without a plan can leave the hip weaker, stiffer, and less prepared for walking. On the other side, pushing through every walk because the pain feels "not that bad" can keep overloading the same tissue.
If your pain is mild, clearly linked to a recent activity spike, and starts to improve with sensible changes, conservative care is often reasonable. If walking is becoming more guarded, pain is spreading, daily tasks are getting harder, or you cannot tell whether the problem is improving, get assessed sooner.
Safety first: Good physical therapy does not mean pushing through pain. It means identifying whether the pattern matches a strain, a load problem, or something that needs broader medical evaluation.
Uncertainty is a reason to get help. In clinic, we would rather screen a problem early than see you six weeks later after the pain has changed the way you walk, exercise, and sleep.
How Our Physical Therapists Pinpoint the Problem
A good evaluation should feel less like a generic workout screen and more like a focused investigation. Front-of-hip pain can come from the muscle itself, the way you walk, nearby joints, or even compensation from another area.
It starts with your story
The first part is conversation, not exercise.
We want to know:
- Where you feel it
- When it started
- Whether it came on suddenly or gradually
- What makes walking worse
- How sitting, stairs, hills, or getting out of the car affect it
- What your recent activity level has looked like
That history often reveals the pattern. A soccer player, a parent getting back into walking, and an office worker with a long commute can all point to the front of the hip, but the underlying causes may differ.
Then we watch you move
Walking is one of the most useful parts of the exam. A gait analysis helps us catch the things patients often cannot feel.
We look for signs such as:
- Shortened stride on the painful side
- Reduced hip extension behind the body
- A trunk lean or backward shift
- Guarding when the leg swings forward
- Compensation through the low back or pelvis
Small movement changes matter. They tell us whether the hip flexor is the main pain generator or whether another restriction is forcing it to work harder.
We test strength and length
Hands-on testing helps identify what tissue is irritated and what capacity is missing.
This usually includes:
- Manual muscle testing: To see whether hip flexion is painful or weak
- Range of motion assessment: To compare both sides
- Palpation: To find tender structures in the front of the hip
- Flexibility screens: Including positions that assess hip flexor length, such as the Thomas test
- Functional tasks: Sit-to-stand, step-up, stair pattern, or single-leg control
These findings matter because treatment differs depending on the pattern. A very tight hip flexor needs a different entry point than a painful but weak one. A runner with poor pelvic control needs something different than a commuter who mainly hurts after sitting.
We also rule out look-alikes
Not every case of hip flexor pain when walking is a hip flexor problem.
Front-of-hip pain can overlap with:
- joint irritation
- lumbar referral
- tendon irritation
- abdominal or groin involvement
- compensation from knee or foot mechanics
That is why a one-size-fits-all handout rarely solves the issue.
What you should leave with
A strong PT evaluation should give you three things right away:
- A working diagnosis
- Clear aggravating factors
- A plan for what to do this week
You should not leave wondering whether you are supposed to rest completely or “just stretch it.” You should know what movements to modify, what exercises fit your current stage, and what signs would change the plan.
Your Evidence-Based Recovery Plan
Recovery works best when it follows a sequence. Calm the irritation. Restore mobility where it is missing. Build strength. Retrain the movements that keep provoking pain. Then return to your normal walking, workouts, or sport with enough capacity to stay there.
What usually does not work
People often try to solve hip flexor pain when walking with one tool only. They stretch a lot. Or they rest until they feel better, then jump back into activity. Or they get a quick massage, feel temporary relief, and assume the problem is fixed.
Those approaches can help symptoms, but they often miss the full picture.
A useful comparison for patients deciding between symptom relief and a broader rehab plan is this article on Physiotherapy Vs Massage. Massage can reduce short-term discomfort. Physical therapy aims to pair symptom relief with movement correction and progressive loading.
Pillar one is reducing irritation
Early treatment is not about doing nothing. It is about stopping the repeated overload that keeps the tissue angry.
That may include:
- Temporary activity modification: Shorter walks, fewer hills, less speed
- Hands-on treatment: Soft tissue work to the front of the hip and nearby structures
- Joint or pelvic mobility work: If restricted motion is shifting load forward
- A short-term gait adjustment: Sometimes a smaller stride or cadence cue reduces pain while the tissue calms
This is also where education matters. Patients often feel better when they understand why a long uphill walk hurts more than a flat one, or why getting up after sitting is such a common trigger.
Pillar two is restoring strength and control
An effective PT protocol emphasizes gradual eccentric loading progression. A key benchmark for return to activity is achieving more than 80% symmetric hip flexion strength compared with the other side, and a strength deficit greater than 20% is linked to a 2.5 times higher risk of reinjury. That benchmark comes from the clinical guidance summarized by Alexander Orthopaedics, discussed earlier in the gait section.
In plain terms, the hip has to do more than feel better. It has to tolerate load again.
A progression may include:
- Isometric hip flexion holds: Useful when resisted motion is painful
- Controlled lowering drills: To build eccentric tolerance
- Core work: To reduce extra strain through the pelvis and low back
- Glute strengthening: So the front of the hip does not do all the work
- Single-leg stability work: To prepare for stairs, hills, and faster walking
For patients who want a broader home program, our article on hip pain relief exercises can complement a personalized plan.
Pillar three is fixing the movement pattern
This part is often the difference between short-term relief and lasting improvement.
If your stride stays guarded, your pelvis stays tipped forward, or your body keeps borrowing motion from the low back, the front of the hip may continue to flare even after it gets stronger.
Gait retraining may focus on:
- Step length
- Cadence
- Pelvic control
- Hip extension behind the body
- Reducing protective limping
At this stage, some patients also benefit from options such as dry needling, aquatic therapy, or a structured return-to-walk progression offered in outpatient rehab settings. Peak Physical Therapy and Sports Performance provides those services across South Shore locations as part of individualized plans for orthopedic and sports-related hip pain.
What works best: The right dose at the right time. Too little loading leaves the hip deconditioned. Too much too soon recreates the problem.
Sample Hip Flexor Strengthening Progression
| Phase | Exercise Example | Goal |
|---|---|---|
| Early pain-management phase | Supine isometric hip flexion hold, gentle heel slides, supported marching | Calm symptoms and restore comfortable basic movement |
| Early loading phase | Seated march with control, low-range resisted hip flexion, bridge variations | Rebuild tolerance to muscle activation without flare-up |
| Mid rehab phase | Slow lowering from hip flexion, step-ups, standing march with band resistance | Improve eccentric control and pelvic stability |
| Advanced phase | Single-leg balance with march, walking drills, stair and hill progression | Prepare for normal walking demands and daily activity |
| Return-to-activity phase | Sport- or goal-specific drills such as longer walks, incline tolerance, jogging progression if appropriate | Return to activity with better capacity and lower reinjury risk |
The trade-off patients need to understand
There is no prize for going from painful walking to a full return in one leap. The hip flexor responds better to steady exposure than dramatic spikes.
That means:
- a little less “testing it”
- more consistent exercise
- fewer all-or-nothing weeks
- and clearer progression criteria
That is especially important for desk workers returning to activity. If the front of the hip has been shortened and underloaded for months, the answer is not endless stretching. It is progressive capacity building.
Start Your Journey to Pain-Free Walking on the South Shore
Hip flexor pain when walking can make you second-guess a lot of ordinary things. Your commute. Your workouts. Even a short walk around the neighborhood. But once the pattern is identified, the path forward usually becomes much less confusing.
If your symptoms are coming from a strain, tightness, deconditioning, or a movement problem, the right rehab plan can help you stop compensating and start rebuilding normal walking again. If your symptoms point to something else, a thorough evaluation helps you move in the right direction sooner.
Why acting early helps
The earlier you address a front-of-hip problem, the easier it is to correct the movement changes that develop around it. Waiting often means the body adds extra strategies like limping, trunk lean, low back tension, or reduced stride length. Those patterns can keep pain going longer than the original irritation.
If your walking already feels off, it may also help to learn more about how to improve gait so you can understand why small changes in movement matter so much.
Care close to home
For South Shore residents, access matters. Whether you live near Quincy, Hanover, Plymouth, Scituate, Weymouth, Braintree, Duxbury, Norwell, Kingston, Pembroke, Milton, Cohasset, or East Bridgewater, getting evaluated locally makes it easier to stay consistent with rehab.
A physical therapy visit should leave you with clarity, not more uncertainty. You should understand what is causing your pain, what to stop doing for now, what to start doing today, and how you will safely progress back to the activities that matter to you.
Bottom line: You do not have to accept front-of-hip pain as part of getting older, getting back into shape, or getting through another busy season.
If every walk reminds you that something is off, get it looked at. A targeted plan can make daily movement feel normal again.
If hip flexor pain when walking is limiting your routine, Peak Physical Therapy and Sports Performance offers in-person evaluations across the South Shore to identify the cause of your pain and build a personalized recovery plan that fits your goals, schedule, and activity level.