One awkward plant, one hard cut, one pop during a game at Braintree High, and your week changes fast. Maybe you're still waiting on imaging. Maybe surgery is already scheduled. Maybe you've had reconstruction and now you're home with a swollen knee, a brace, and a long list of questions.
That's usually where people start searching for ACL recovery physical therapy Braintree MA. They want a plan that feels local, practical, and clear. They want to know when they'll walk normally, when the swelling settles, what matters in rehab, and how to avoid going through this twice.
Around the South Shore, an ACL tear affects more than sports. It changes your commute, stairs, workday, sleep, errands, and the simple confidence of moving without thinking. The good news is that ACL rehab is not guesswork when it's done well. It follows a phased, criteria-based process that protects the graft, rebuilds strength, and prepares you for real life again.
Table of Contents
- Your ACL Recovery Journey Starts Here in Braintree
- The First Six Weeks Controlling Swelling and Restoring Motion
- Building a Stronger Foundation Weeks 6 to 12
- Advanced Training for Your Return to Sport Months 3 to 9
- Winning the Mental Game and Preventing Future Injury
- Take the Next Step at Peak Physical Therapy in Braintree
Your ACL Recovery Journey Starts Here in Braintree
It often starts the same way. You twist, hear a pop, or feel the knee give out. A day later, you are trying to figure out how to get through work, drive down Granite Street, climb stairs at home, and make sense of a recovery timeline that suddenly feels much bigger than the injury itself.

That first stretch is where good guidance matters. Some Braintree patients come to us right after the injury. Others arrive after surgery. Some are high school athletes trying to get back for a season. Others want to coach, chase their kids at Sunset Lake, or return to gym workouts without feeling unstable. The plan changes based on your goals, graft type, swelling, pain, schedule, and insurance rules, but the overall path is still clear.
A strong ACL rehab plan answers practical questions early. What needs protection right now? What motion has to come back first? How much loading can the knee tolerate this week? What testing will show that you are ready for running, cutting, or full sport later on?
For Braintree residents, local care also solves local problems. Commutes into Boston, school pickup, winter weather, and South Shore traffic can all affect how often you can get in. We build plans that fit real life, not an ideal calendar. That includes helping you understand visit frequency, home exercise priorities, and how to use your appointments well if your insurance limits visits or requires referrals.
One of the first things I tell patients is simple. Your timeline matters, but your criteria matter more. Two people can both be four months out from surgery and need very different rehab that week. One may be ready to start higher-level strength work. The other may still be working through swelling, quad control, or confidence on stairs.
If the knee is still puffy later in the day, that is useful information. If you are not sure what is normal and what needs attention, our guide on how to reduce knee swelling after injury or surgery can help you sort out the basics between visits.
Local recovery means local problem-solving
At Peak Physical Therapy in Braintree, we map recovery in phases so you always know what the current job is. Early rehab focuses on calming the knee and restoring motion. The middle phase builds strength and control. Later rehab adds impact, change of direction, and return-to-sport testing. Along the way, we coordinate with your surgeon when needed and adjust for the demands of your actual life, whether that means getting back to hockey, soccer, lifting, or a long shift on your feet.
Progress should feel organized. Each visit should tell you what improved, what still needs work, and what the next target is.
The shape of the road ahead
Here is the big-picture roadmap we use in Braintree:
- Early phase: reduce swelling, restore full knee extension, re-establish a clean walking pattern
- Foundation phase: build quad and hip strength, improve balance, and clean up movement mechanics
- Performance phase: add running, jumping, landing, and controlled cutting when the knee shows it is ready
- Return phase: use strength, hop, movement, and confidence testing to decide what activities are safe to resume
That structure gives patients something they usually need right away. A clear plan, measurable checkpoints, and a clinic team that can help them handle both the rehab work and the scheduling details that come with recovering in Braintree.
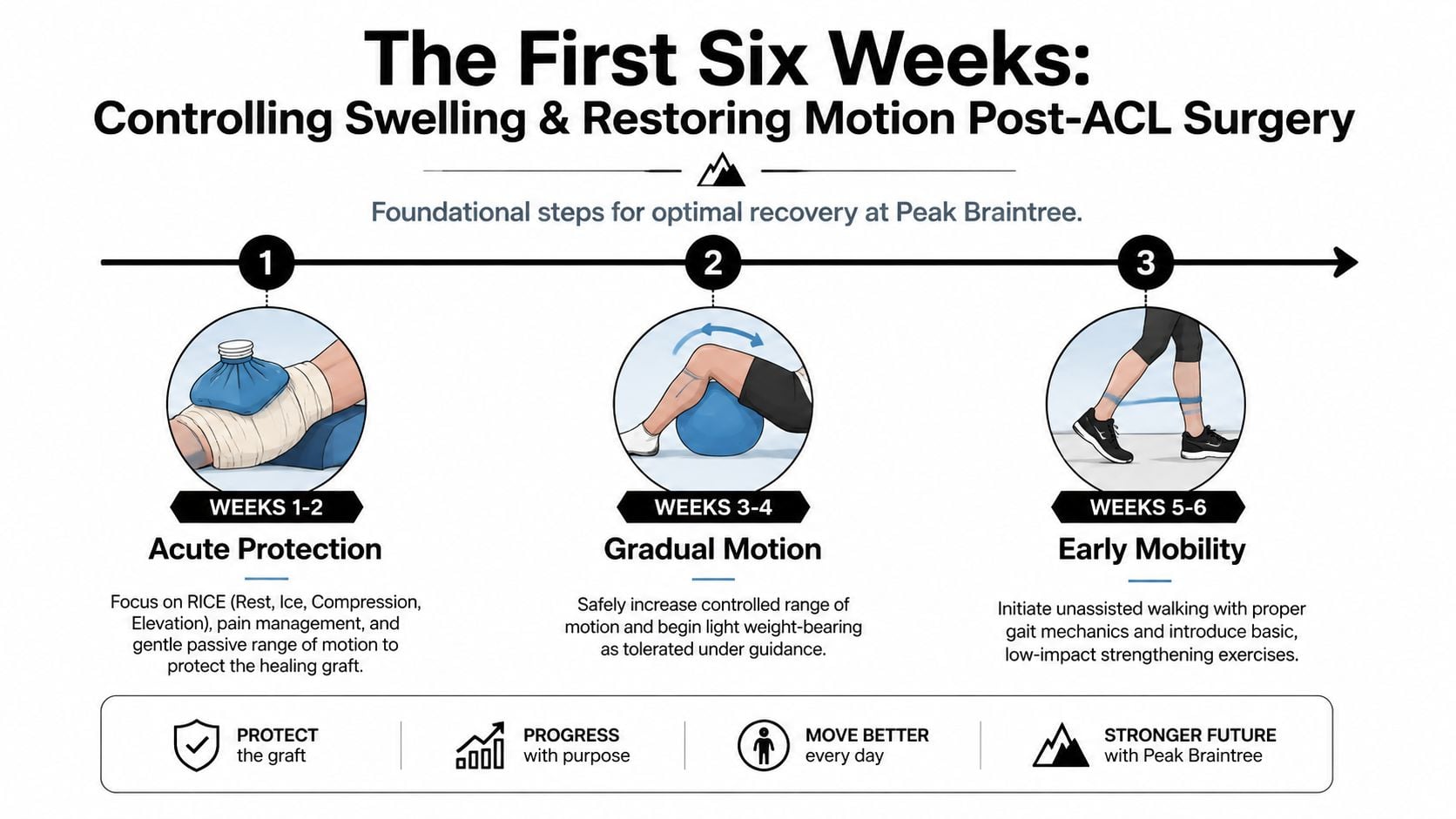
The First Six Weeks Controlling Swelling and Restoring Motion
You had surgery, the brace is on, and everyone around you wants to know when you will be back to normal. In Braintree, that can mean getting back to work, driving comfortably, managing stairs at home, or keeping up with family routines on the South Shore. In the first six weeks, the better question is simpler. Can the knee calm down, straighten fully, and start accepting normal movement again?
What matters most right away
The early phase sets the tone for everything that follows. A swollen, stiff knee is harder to strengthen. A knee that does not fully straighten often changes how you walk, how the quad works, and how comfortable the joint feels day to day.
Early on, many patients focus on bending because it is easier to notice. Bending matters, but full knee extension usually deserves more urgency. A commonly used hospital-based ACL rehab protocol notes that early loss of extension is tied to a higher risk of arthrofibrosis and a longer recovery timeline for return to sport. That is one reason we keep extension work near the top of the list in Braintree, especially during the first couple of weeks.
Practical rule: If the knee will not fully straighten early, make that a daily priority.
The other problem we watch closely is quad inhibition. After ACL surgery, the thigh muscle often feels like it has gone quiet. Patients try to tighten it and get very little response. That affects walking, stair use, transfers, and knee control. We often use high-intensity NMES along with targeted exercise to help restore a cleaner quad contraction, then we build from there based on how the knee responds.
What your early visits usually include
At Peak Physical Therapy in Braintree, these visits are focused and specific. We are not trying to do everything at once. We are trying to reduce the problems that slow people down later.
Common priorities include:
- Swelling management: Ice, compression, elevation, and hands-on treatment can improve comfort and make motion easier to tolerate. If your knee keeps puffing up between visits, our guide on reducing swelling after injury or surgery gives you a useful home starting point.
- Extension restoration: Heel props, positioning, soft tissue work when needed, and guided exercises help restore full straightening.
- Flexion work: Heel slides and controlled mobility drills help bring back bending without stirring up extra irritation.
- Quadriceps activation: Quad sets, straight-leg raise progressions when appropriate, and NMES help the muscle join the work again.
- Gait practice: Crutches and a brace are only part of the picture. We also clean up the walking pattern so you do not build a limp that hangs around longer than it should.
Here is how this phase often looks in the clinic:
| Timeframe | What patients notice | What we focus on |
|---|---|---|
| Weeks 1 to 2 | Swelling, pain, difficulty lifting the leg | Protection, extension, basic muscle activation |
| Weeks 3 to 4 | Better tolerance to movement, but stiffness remains | Range of motion, gait quality, swelling control |
| Weeks 5 to 6 | More daily confidence, but clear weakness | Cleaner walking, early strength, movement quality |
There are trade-offs in this stage. Push too hard on motion and the knee can get more irritable. Stay too cautious and stiffness can linger. Good rehab lives in the middle. We adjust the plan visit by visit based on swelling, pain, motion, and how your knee handles daily life.
That local part matters. A patient commuting through Braintree traffic, sitting through long workdays, or trying to get back to errands too quickly often sees swelling rebound by evening. We plan for that. Sometimes the right move is adding work. Sometimes it is changing timing, reducing irritation, and spacing exercises better through the day.
We also help with the practical side. Early after surgery, missed visits can slow progress, so our Braintree team works to keep scheduling consistent and coordinate around work and family demands. If insurance limits visits or requires authorizations, we help you handle those details early so treatment stays on track.
Building a Stronger Foundation Weeks 6 to 12
Around week 7 or 8, a lot of Braintree patients tell us the same thing. The knee feels better, stairs are getting easier, and it is tempting to do more because daily life is starting to look normal again. That is usually the point where good progress can either build momentum or get sidetracked by swelling, poor mechanics, and too much activity too soon.

We build strength on top of control
This phase is less about getting the knee to move and more about getting the leg to work. The quadriceps need to produce force again. The hip and trunk need to keep the knee in a good position. Walking, step-downs, and single-leg work should look controlled, not rushed or uneven.
At Peak in Braintree, we do not progress exercises just because the calendar says week 10. We look at how the knee responds after sessions, whether swelling stays settled, how well you control body weight on one leg, and whether your movement stays clean when the work gets harder. Those details matter because strength built on compensation does not hold up well later.
A patient who is back at the office, sitting through long stretches, then trying to squeeze in workouts after fighting Route 3 traffic often needs a different plan than a high school athlete on a school vacation schedule. Both can make strong progress. The weekly setup has to match real life.
What usually changes from weeks 6 to 12
By now, rehab should start looking and feeling more athletic, even for patients whose main goal is daily function. We are still protecting the knee. We are also asking more from it.
Common focus areas include:
- Strength training: squats, split squats, step-ups, leg press variations, and controlled hamstring work
- Single-leg control: balance progressions, step-down patterns, and reach tasks that expose side-to-side differences
- Movement quality: keeping the knee from drifting inward and limiting trunk shift during loaded tasks
- Conditioning: bike, sled, or other low-impact options that rebuild work capacity without stirring up the joint
For some patients, this is also the right time to layer in more structured sports performance training programs once the basics are in place and the knee is tolerating strength work well.
Signs the knee is ready for more, and signs to slow down
Good progress in this window is usually pretty clear in the clinic and at home.
| Green lights | Yellow lights |
|---|---|
| Swelling stays fairly stable through the week | The knee repeatedly gets puffy after normal activity |
| Walking speed improves without limping | Limp returns when you are tired or distracted |
| Step work looks controlled | The knee drops inward or you unload the surgical side |
| Strength work is hard but repeatable | Every session causes soreness that lingers or builds |
Those yellow lights do not mean something is wrong. They mean the dose needs to change. Sometimes we reduce depth, simplify a single-leg drill, or spread exercises out differently across the week. Sometimes we push harder because the knee is ready. Good ACL rehab requires both judgment and adjustment.
The mistakes that slow people down
The biggest problem in this phase is not usually lack of effort. It is misplaced effort.
Patients often lose time by doing advanced exercises before they can control simpler ones. A shaky single-leg squat does not improve because we add speed. It improves when strength, alignment, and repetition quality get better first.
Another common issue is underloading the leg because the knee still feels unfamiliar. That protective habit is understandable, but it can keep the surgical side weak. We coach patients to load the leg with purpose and within tolerance, then reassess based on how the knee responds later that day and the next morning.
Scheduling matters here too. If your insurance requires visit limits, authorizations, or a specific referral sequence, our Braintree team helps you handle that early so the middle phase of rehab does not get interrupted right when progression should be picking up.
For South Shore patients, this is the stretch where confidence starts to return. Strength has to return with it.
Advanced Training for Your Return to Sport Months 3 to 9
A Braintree athlete often hits this phase feeling close to normal. The knee is less swollen, daily walking is easier, and stairs are not the same challenge they were a few months ago. Then the real question shows up. Can the knee handle a hard cut at practice, a fast stop on the court, or a sprint after a loose ball without compensation?

What we measure before higher level drills
At this stage, feeling better is helpful, but it is not enough to clear someone for jumping, cutting, pivoting, or full-speed practice. Return-to-sport decisions should be based on objective testing and movement quality. A consensus statement on return to sport after ACL injury describes a criteria-based process that includes strength testing, hop performance, movement assessment, and sport-specific progression rather than time alone.
In the clinic, we look for more than whether a patient can complete a drill once. We want to see whether the surgical leg can produce force, absorb force, and repeat the task cleanly without loss of control as fatigue builds.
A typical late-stage testing battery may include:
- Strength testing: checks whether the involved leg is still lagging in quad or hamstring force
- Hop testing: examines distance, symmetry, landing control, and confidence on one leg
- Movement assessment: looks for knee valgus, trunk compensation, shortened stance time, or hesitation
- Agility progression: shows how the knee responds to acceleration, deceleration, and direction change
Those benchmarks matter in real life on the South Shore. A high school soccer player in Braintree, a weekend basketball player in Quincy, and a parent coaching youth sports in Weymouth all need more than a stable knee on level ground. They need control at speed.
How we build the return-to-sport progression at Peak in Braintree
Months 3 to 9 are rarely a straight line. One week may focus on force production. The next may expose a landing problem, a timing issue, or a confidence gap during reactive drills. Good rehab in this phase means adjusting the plan without losing momentum.
Our progression usually follows this order:
| Level | What the knee must handle |
|---|---|
| Foundational power | Jumping and landing with good alignment and load acceptance |
| Running progression | Jogging, then building pace and tolerance without swelling spikes |
| Multi-directional loading | Lateral movement, stopping, and direction changes under control |
| Reactive sport demand | Cutting, pivoting, and responding to unpredictable cues |
The trade-off is simple. Progress too slowly and strength, power, and confidence stall. Progress too fast and the knee may get irritable, mechanics may slip, and compensation patterns can stick. Our job is to dose the work correctly, then recheck how the knee responds later that day and the next morning.
For athletes and active adults who want extra work after they clear the right rehab milestones, Peak also offers sports performance training in Massachusetts to help improve speed, power, and movement quality after injury.
Sport-specific work has to match the person, not just the protocol
A return-to-sport plan for a football player does not look the same as a return-to-running plan for a South Shore road racer or a return-to-duty plan for someone with a physical job. The demands are different. The progression should be different too.
For field and court athletes, we often add deceleration drills, change-of-direction work, and reactive cueing before any full return to scrimmage or competition. For patients who play soccer or football, education around mechanics and exposure matters, and resources on how footballers can avoid knee damage can reinforce what we coach in the clinic.
Insurance and scheduling can affect this phase more than people expect. If visits require authorization or your plan limits how often you can come in, our Braintree team helps you organize appointments around the highest-value sessions so testing, progression, and return-to-play decisions do not get delayed right when the work becomes more specific.
The goal in months 3 to 9 is not to hope the knee is ready. The goal is to show that it is ready.
Winning the Mental Game and Preventing Future Injury
You get cleared for harder cutting and jumping work. Then your foot hits the floor, your knee feels stable, and you still hesitate for half a second. That moment is common after ACL rehab, and it matters.
Physical recovery and mental readiness do not always line up on the same day. We see that in Braintree with high school athletes, weekend basketball players, and adults who just want to get back to running along the South Shore without second-guessing every pivot or uneven step. Confidence has to be rebuilt on purpose.
Why confidence needs objective testing and real practice
Fear usually drops when the knee keeps passing harder tasks without swelling, pain, or loss of control. That is why we do not treat confidence like a pep talk problem. We treat it like a rehab problem. We build it with exposure, repeatable movement quality, and clear benchmarks.
Research on ACL return to sport has shown that psychological readiness plays a meaningful role in whether athletes return to their prior level of play and how they perform once they do, as reviewed in the British Journal of Sports Medicine discussion of psychological factors after ACL reconstruction. In the clinic, that shows up in simple ways. A patient trusts the knee more after they land cleanly, repeat the rep without guarding, and handle the same task again once they are a little tired.
At Peak in Braintree, we use that progression deliberately. We do not ask you to just "trust it." We show you why the knee is earning trust.
That also helps families and athletes make better decisions outside the clinic. If you are returning to a cutting sport, general injury education like how footballers can avoid knee damage can reinforce the mechanics and risk patterns we coach during rehab.
Prevention starts before discharge
The best injury prevention plan is built into the later phases of ACL rehab, not saved for the end. Once strength is coming back, the focus shifts to how you absorb force, slow down, change direction, and react when attention is split. Those are the moments when old compensations tend to creep back in.
We watch for the trade-offs that matter in real life. A patient may test strong on a machine but still collapse inward during a single-leg landing. Another may move well in a quiet treatment space but lose control when speed, fatigue, or decision-making gets added. Those details help explain why some people feel "done" on paper but not ready for a full return.
A few habits make a big difference after formal rehab ends:
- Keep single-leg strength work in the program
- Practice deceleration, not just acceleration
- Build workload gradually instead of cramming activity into one weekend
- Pay attention to hesitation, especially during cutting or landing
- Return for retesting if the knee feels off after a jump in activity
For many local patients, prevention also depends on staying consistent after discharge. Busy work weeks, school schedules, and youth sports calendars in Braintree can interrupt that rhythm fast. Our team helps patients set up a plan they can effectively follow, and if you are still comparing care options, our guide to physical therapy in Braintree, MA gives a practical overview of what to expect.
The strongest return is the one that holds up in the gym, on the field, at work, and during a normal week on the South Shore.
Take the Next Step at Peak Physical Therapy in Braintree
A lot of ACL recoveries stall before rehab really starts. The knee is sore, the calendar fills up, insurance questions pile on, and it becomes easy to lose the first couple of weeks that matter most.
The better plan is simple. Get your evaluation scheduled early, know what your first month should look like, and set up a visit rhythm you can realistically keep. For many people in Braintree and across the South Shore, that means choosing appointment times that fit work, school pickup, train schedules, or help at home if driving is limited.
If you already had surgery, bring the operative note or discharge paperwork if you have it. Bring your brace, your medication list, and any instructions from your surgeon. If surgery is still ahead, ask about prehab. In the clinic, we often see that patients who start with better motion, less swelling, and stronger quad control have an easier time in the early post-op phase.
Before the first visit, handle a few practical details:
- Insurance and referrals: check whether your plan requires a referral or authorization and what your out-of-pocket cost will be
- Scheduling: book more than one visit at a time so your progress does not get interrupted by a busy week
- Home setup: have a clear space for exercises, a place to raise the leg, and ice ready to use
- Transportation: make a backup plan if you cannot drive yet, especially in the first couple of weeks
It also helps to ask good questions when you call. Ask how the evaluation is structured, how progress is measured, how often reassessment happens, and how the clinic communicates with your surgeon if your swelling, pain, or motion is not tracking as expected.
Some patients also ask about advanced rehab options such as blood flow restriction training. That can be useful in the right phase and for the right patient because it allows lower-load strength work when the knee is not ready for heavier loading yet. We decide that based on the knee in front of us, not on a template.
If you want a clearer sense of clinic access and what care looks like locally, our guide to physical therapy in Braintree, MA gives a practical overview. Peak Physical Therapy and Sports Performance is located at 501 John Mahar Hwy, Suite #200 in Braintree, which is convenient for patients coming from town and nearby South Shore communities.
The next step is an evaluation with a plan that fits your life. We help patients set up the schedule, sort through insurance questions, and build an ACL rehab roadmap they can follow.