You notice it on the first few steps out of bed. Then again walking the seawall, standing on the sidelines at a youth soccer game in Pembroke, or pushing through your commute into Quincy. Foot pain has a way of shrinking your world fast. People start skipping beach walks, cutting workouts short, and planning their day around how much standing they can tolerate.
That kind of slowdown is common, but it shouldn't become your new normal. On the South Shore, we see how foot pain affects real routines: long days on your feet at work, weekend runs near World's End, errands in Plymouth, and family time that doesn't pause because your heel or arch is flaring up. The good news is that there are practical, evidence-based ways to calm pain, restore movement, and help you trust your foot again.
Table of Contents
- Dont Let Foot Pain Sideline Your South Shore Life
- What to Expect at Your First Foot Pain Visit in Quincy or Plymouth
- Our Proven Treatments for Foot Pain Relief
- Why We Look Beyond Your Foot for Lasting Relief
- Sample Home Exercises for South Shore Residents
- Your Guide to Returning to Activity on the South Shore
- Take the First Step Away from Foot Pain Today
- Frequently Asked Questions About Foot Pain Therapy
Dont Let Foot Pain Sideline Your South Shore Life
A lot of people wait too long to get help because foot pain seems small at first. It's just a sore heel after a walk in Duxbury. A tight arch after pickleball. An ache in the ball of the foot that shows up after coaching, shopping, or chasing kids around the yard. Then it keeps hanging around.

Foot pain is widespread. 81% of Americans experience foot pain, and physical therapy was rated the most effective treatment at 2.299 on a 4-point scale, ahead of over-the-counter medication and stretching in the 2025 Foot Pain Trends Report. That matters because many people try to push through, switch shoes, or rest for a few days without ever addressing why the problem started.
Common South Shore stories we hear
In clinic, the pattern is familiar:
- The walker: Someone who loves morning laps near Nantasket Beach but now cuts the route short because the first mile hurts.
- The parent coach: A Pembroke or Hanover parent who can handle practice, but the next morning their heel throbs.
- The runner: A local runner training on roads, trails, or neighborhood loops who notices pain building with each week of mileage.
- The worker on their feet: A person whose job doesn't allow much sitting, so symptoms build by lunchtime and linger into the evening.
These aren't dramatic injuries every time. Often it's accumulated stress, stiffness, weakness, or a change in activity that the foot hasn't handled well.
Foot pain changes more than exercise. It changes how you work, shop, commute, and show up for the people around you.
Why physical therapy helps
The goal of physical therapy for foot pain isn't to chase symptoms from one week to the next. It's to identify what's overloaded, what's too stiff, what's too weak, and what movement pattern keeps feeding the problem. That could involve the foot itself, but it can also involve the ankle, calf, knee, hip, or the way you walk.
Around the South Shore, people don't need a generic handout. They need care that fits the life they are striving to return to, whether that's standing comfortably at work in Weymouth, running in Cohasset, or walking downtown Plymouth without thinking about every step.
What to Expect at Your First Foot Pain Visit in Quincy or Plymouth
Your first visit should feel organized, practical, and specific to you. Good foot pain treatment starts with listening before it starts with exercise. We want to know where it hurts, when it started, what makes it worse, what you've already tried, and what you're trying to get back to.
For many people, the bigger concern is simple: "Is this something I can fix, or am I going to keep dealing with it?" That question shapes the visit. Physical therapy has an overall success rate of 68-72% for pain relief, patients often see a 40-50% reduction in pain intensity after 4-6 weeks of consistent treatment, and 88% report high satisfaction with outcomes, according to this summary of physical therapy success rates for pain relief. Those numbers don't replace a personal evaluation, but they do tell people this approach is worth taking seriously.
We start with your story
The first part of the session usually sounds more like a conversation than a test. Your therapist asks about:
- Your daily demands: standing at work, walking the dog, climbing stairs, commuting, lifting, coaching, or caring for family
- Your routine before pain started: running, gym work, court sports, beach walks, or just being able to move through the day without thinking about your foot
- What you've noticed: morning pain, pain after activity, swelling, numbness, stiffness, or pain that shifts into the ankle, calf, knee, or hip
Those details matter. Heel pain first thing in the morning points us one direction. Pain that ramps up after long standing or hard workouts may point another.
Then we look at how you move
A thorough exam goes beyond the sore spot. We watch how you stand, walk, squat, balance, and transfer weight. We assess the foot and ankle, but we also screen the chain above it because movement problems rarely stop at one joint.
A first visit often includes:
- Gait observation to see how your foot loads and pushes off
- Mobility testing of the foot, ankle, and calf
- Strength testing in the foot, lower leg, and often the hips
- Balance and control work to see how stable you are on one leg
- Palpation and hands-on assessment to identify irritated tissue and joint stiffness
Practical rule: If a provider only looks at the exact painful spot and ignores how you walk, that's rarely a complete foot pain evaluation.
You leave with a plan, not a guess
By the end of the visit, you should understand what the problem appears to be, what the short-term priorities are, and what the plan looks like over the next few weeks. That might include activity modifications, a few starter exercises, hands-on treatment, and guidance on what not to do yet.
The plan should match your real goal. Someone trying to get through a retail shift in Braintree needs a different progression than someone aiming to get back to longer runs in Plymouth. The evaluation should make that clear from day one.
Our Proven Treatments for Foot Pain Relief
Foot pain responds best when treatment matches the driver of the problem. A sore heel from overload needs a different approach than a stiff foot after an ankle injury, and both are different from pain that keeps returning because walking mechanics never changed. The work in clinic is targeted. Not random. Not just a sheet of stretches.
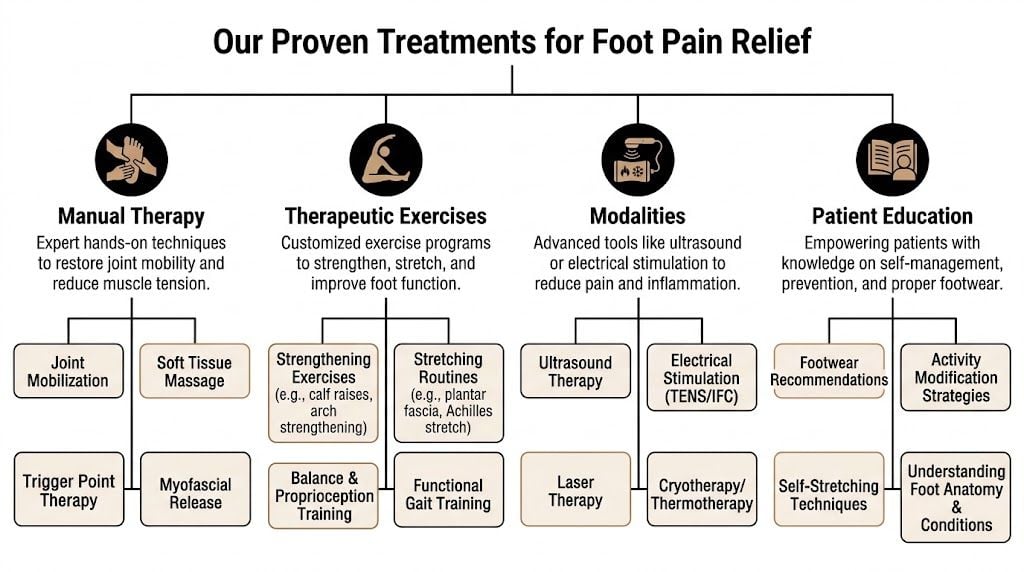
Hands-on care that changes how the foot moves
Manual therapy is often useful when the foot and ankle aren't moving well, or when irritated tissue needs help calming down so you can tolerate exercise. That can include soft tissue work, joint mobilization, taping, or more specific techniques based on the pattern we find.
One option is instrument-assisted soft tissue mobilization, sometimes called IASTM. According to this overview of how a physical therapist approaches foot pain treatment, these tools apply controlled pressure to tissue and may reduce forefoot pronation by 15-25% after a session, which can improve tissue glide and reduce strain through the plantar fascia. That's not a magic fix, and it isn't the answer for every case, but it can be helpful when tissue restriction is part of the problem.
What doesn't work well is relying on passive treatment alone. Hands-on care can open the door. It doesn't keep the door open unless strength and movement control improve too.
Exercise that matches the problem
The right exercise plan is usually key to real change. It does more than stretch a painful area. It restores load tolerance so daily activity stops irritating the foot every time you use it.
A useful program often includes a mix of:
- Mobility work: ankle and calf motion can affect how the foot absorbs load
- Foot and lower leg strengthening: the small muscles in the foot and the calf complex often need more capacity
- Single-leg control: balance, step-downs, and controlled loading build the stability people need for hills, stairs, and uneven ground
- Progressive loading: tissues improve when load is introduced in the right amount, not when everything is avoided for too long
Some people need less stretching than they think. Others are doing the right exercise at the wrong intensity. That's a common reason pain lingers.
Gait work and activity-specific retraining
Many foot pain cases return because the original movement pattern never changed. Someone may feel better on the table, then go right back to overstriding, collapsing through the arch, or pushing off a stiff ankle. The symptoms settle for a week or two, then come back.
That's where gait training matters. We look at walking and, if appropriate, running mechanics. We help patients change how they load the foot during real tasks. For a South Shore resident, that may mean improving tolerance for beach walking, standing at youth sports events, climbing train station stairs, or returning to neighborhood runs.
If you'd like a closer look at one technique often used for stubborn symptoms, our article on dry needling for foot pain benefits and success rates explains where it can fit into a broader plan.
Passive care can reduce symptoms. Movement retraining is what helps many people keep those symptoms from returning.
Specialized options when they fit
Some people benefit from additional tools, but they should be used for a clear reason.
A few examples:
| Approach | When it may help | What to know |
|---|---|---|
| Dry needling | Irritable calf or foot muscles, trigger points, guarded tissue | Often paired with exercise and mobility work, not used as a standalone fix |
| Aquatic therapy | Painful weight bearing, post-surgical recovery, lower tolerance for land exercise | Lets people start moving with less stress through the foot |
| Taping or temporary support | Early irritation, short-term unloading, activity transitions | Helpful for symptom control, but not a replacement for building strength |
| Footwear guidance | Pain linked to shoe choice, workload, or poor support for current activity | Useful when tied to your exam findings and daily routine |
Peak Physical Therapy and Sports Performance meets the needs of South Shore patients who want local access to services such as dry needling, aquatic therapy, gait training, and orthopedic rehabilitation in the communities where they already live and work.
What works better than quick fixes
People are often surprised by what doesn't help much long term:
- Only resting until pain settles: this can reduce irritation, but it doesn't build capacity
- Only changing shoes: footwear can matter, but shoes don't correct weakness, stiffness, or movement errors by themselves
- Only stretching the foot: many cases need strength and load progression more than endless stretching
- Jumping back too fast: symptoms often return when activity increases before tissue tolerance catches up
The best treatment plan combines short-term pain relief with long-term rebuilding. That's how you get from "I can get through the day" to "I can trust this foot again."
Why We Look Beyond Your Foot for Lasting Relief
A lot of people come in convinced the problem lives only in the foot. That's understandable. The pain is there, the tenderness is there, and that's the area everyone talks about. But chronic foot pain often behaves like the end result of a bigger movement problem.

The foot is often the victim, not the cause
When the hip is weak, the knee collapses inward, the pelvis drifts, or the trunk doesn't control load well, the foot often pays for it. That's why we check the whole chain in persistent cases. Studies show that 30-50% of chronic foot pain cases are linked to hip abductor weakness, and patients are 2.5 times more likely to have recurring pain if proximal strength isn't addressed, based on this review of physical therapy for foot pain and proximal strength findings.
That doesn't mean every person with heel pain needs a full-body athletic program. It means good treatment should test whether the body above the foot is contributing. If it is, ignoring it usually keeps the cycle going.
What that means for treatment on the South Shore
For someone walking dunes, sidewalks, turf fields, or uneven trails, control from the hips and core often matters more than they expect. A parent coaching in Pembroke may not need harder calf stretches. They may need better single-leg stability so the foot isn't absorbing every bit of rotational stress. A runner in Cohasset may not need more rest. They may need stronger lateral hip control and cleaner stride mechanics.
Our approach reflects that. We don't just ask, "Where does it hurt?" We ask, "Why is the foot taking more load than it can handle?" For people who want a deeper educational look at biomechanics and orthopedic recovery topics, Highbar Health has broader resources at highbarhealth.com.
If your foot pain keeps coming back, the missing piece may not be in your foot at all.
Weight can also influence how much force the feet and lower joints manage day after day. For readers looking for a practical, broader-health resource on that connection, weight loss strategies for joint pain can be a useful complement to a rehab plan.
If walking mechanics are part of your issue, our guide on how to improve gait gives a helpful overview of what therapists look for and why those changes matter.
Sample Home Exercises for South Shore Residents
Home exercises can help, but they work best as part of a plan built around your diagnosis, irritability level, and daily demands. A runner in Scituate, a teacher in Norwell, and someone recovering after foot surgery in Pembroke shouldn't all do the same program. These are safe starting points for many people, not a substitute for an evaluation.

A few safe starting points
Try these gently. Pain that spikes during or after exercise is a sign to stop and get assessed.
Calf stretch at the wall
Stand facing a wall with one foot back. Keep the back heel down and the knee straight. Lean forward until you feel a stretch in the calf. Breathe and hold, then switch sides. This can help when limited calf length is adding stress lower down.Towel scrunches or short-foot activation
Sit with your foot flat and gently pull a towel toward you with your toes, or lightly draw the arch up without curling the toes aggressively. This works on the smaller muscles that support the foot.Supported heel raises
Hold a counter or chair for balance. Rise onto your toes in a controlled way, then lower slowly. Start with both feet if needed. This helps rebuild calf strength and push-off tolerance for walking.Single-leg balance near a stable surface
Stand on one leg with a hand close to support. Keep the pelvis level and the knee soft. This begins to challenge the control your foot, ankle, and hip need together.
When home exercises are not enough
Home programs run into trouble when people keep guessing. They add more reps because "more must be better," or they stop too early because symptoms eased for a few days. Both can delay progress.
A therapist adjusts the plan based on your response. Sometimes that means reducing the volume. Sometimes it means progressing from simple foot work to step-downs, carries, hills, or return-to-run drills. That's the piece generic online routines miss.
If you're looking for additional support options that bring rehab into the home setting, this at-home orthopedic program may be a useful resource for some patients and families.
Start simple. Move consistently. Progress with a reason, not with impatience.
Your Guide to Returning to Activity on the South Shore
Patients don't just want less pain. They want their life back. They want to walk Wompatuck trails, get through a shift without limping, rejoin a local softball league, or run along familiar roads without wondering when the foot will flare up again.
Why guessing usually backfires
The most common mistake is returning based on hope alone. Pain settles, so activity jumps right back to previous levels. Then the tissue gets overloaded before strength, mobility, and control are ready. That cycle is why "I rested and it came back" is such a common story.
A guided progression works better because it gives you a sequence. In a randomized clinical trial on plantar heel pain, structured care followed a 3-phase progression of pain modulation, strengthening, and then functional gait training with load progression. That approach supported return to activity in 8-12 weeks for 85% of cases, as described in this plantar heel pain physical therapy trial.
How we build the return
The return is usually based on what your foot can tolerate, not just what you miss doing. A practical progression often looks like this:
- Settle the irritation so walking and standing become more manageable.
- Build capacity in the foot, calf, and supporting chain.
- Rehearse the task with smart modifications before full volume returns.
For a runner, that may mean controlled walk-run intervals before longer mileage. For a parent coach, it may mean tolerating a practice field and then a tournament day. For a commuter, it may mean handling stairs, parking lots, and a full workday before adding weekend recreation.
If your goal includes running again, our article on running physical therapy explains how therapists bridge the gap between pain reduction and real training.
The biggest advantage of a structured return isn't speed alone. It's confidence. When progress is measured and the next step makes sense, people stop second-guessing every ache and start moving forward again.
Take the First Step Away from Foot Pain Today
Foot pain has a way of stealing ordinary parts of life first. The walk you enjoy. The errands you don't think twice about. The ability to stand, coach, commute, exercise, or keep up with your family without planning around discomfort.
The encouraging part is that foot pain is often very treatable when care goes beyond the sore spot. The most useful plans combine a careful evaluation, hands-on treatment when needed, focused strength work, gait and movement retraining, and a return-to-activity strategy that matches real life on the South Shore. That might mean getting back to beach walks in Scituate, training in Quincy, working on your feet in Braintree, or moving around Plymouth without guarding every step.
Local access matters too. When your care is close to home, it's easier to stay consistent, ask questions, and progress without your rehab becoming another burden on your schedule. With clinics across the South Shore, from Milton to Kingston and beyond, getting started can be simpler than people expect.
If foot pain has been lingering, flaring up, or changing how you live, now is a good time to address it directly instead of waiting for the next setback.
Frequently Asked Questions About Foot Pain Therapy
Do I need a referral to start physical therapy in Massachusetts
In many cases, no. Massachusetts offers Direct Access, which means you can often begin physical therapy without first getting a physician referral. Insurance rules can vary, so it's still smart to verify your specific plan before the first appointment.
How long does foot pain therapy usually take
That depends on the condition, how long you've had it, how irritable it is, and how consistently you follow the plan. Some people improve quickly, while others need a longer progression because they want to return to higher-demand activities.
Will physical therapy replace seeing a podiatrist
Not always. Physical therapists and podiatrists often help in complementary ways. A podiatrist may evaluate medical or structural concerns, while physical therapy focuses on movement, strength, load management, and return to activity.
What should I wear to my appointment
Wear comfortable clothes that let you move easily and shoes you commonly use for walking, work, or exercise. If you have a pair that seems to trigger symptoms, bring that too.
Is it okay to keep exercising with foot pain
Sometimes yes, but it depends on the pattern. Full rest isn't always necessary, and full activity isn't always wise. A therapist can help you modify activity so you stay moving without continuing to overload the irritated area.
What if I've already tried stretches and better shoes
That's common. Those changes can help some people, but they often aren't enough when the underlying issue involves load tolerance, gait mechanics, calf strength, balance, or hip control. That's where a more complete rehab plan tends to make the difference.
If you're ready to stop planning your life around foot pain, book an evaluation with Peak Physical Therapy and Sports Performance. With convenient South Shore locations and personalized care built around how you live, work, and move, it's a practical next step toward getting back on your feet.