You leave the orthopedic visit with a surgery date on the calendar and a head full of questions. You want the pain gone, but you’re also thinking about real life on the South Shore. Can you get up the stairs in your Milton home? Walk Nantasket without that deep ache? Get back to golf in Pembroke, gardening in Duxbury, or just sleeping through the night without shifting every half hour?
That mix of relief and anxiety is normal. Hip surgery rehab asks a lot of you in a short stretch of time, and many individuals don’t get much useful guidance beyond a packet of precautions and a few generic exercises. The missing piece is usually context. Your recovery needs to fit your home, your routine, your surgical approach, and your goals.
That matters because hip replacement is now a routine part of orthopedic care, and outcomes can be excellent. Hip replacement is described as one of the most successful interventions in modern medicine, and procedures for patients age 45 and over rose from 138,700 in 2000 to over 310,800 by 2010, while average hospital stay dropped to just under 4 days as rehab improved, according to this hip replacement outcome summary. If you’re still sorting through symptoms before surgery, it can also help to spend a few minutes understanding various hip pain conditions so the whole process feels less mysterious.
Table of Contents
- Your Hip Surgery Journey on the South Shore Begins Here
- Preparing for Success Your Pre-Hab Plan in Braintree and Beyond
- The First Weeks Navigating Early Recovery at Home
- Your Rehab Roadmap The Phases of Physical Therapy at Peak
- Not All Hip Surgeries Are the Same How Your Rehab Changes
- Getting Back to Your Life Timelines for Driving Sports and Work
- Your Local Partner Peak PT in Quincy Plymouth and Across the South Shore
- Frequently Asked Questions About Hip Rehab
Your Hip Surgery Journey on the South Shore Begins Here
For a lot of South Shore patients, the decision doesn’t happen all at once. It builds over months or years. First it’s avoiding the longer walk at the beach. Then it’s using the railing on every staircase. Then it’s passing on things you’d normally say yes to because you don’t trust the hip.
The encouraging part is that surgery usually isn’t the end of independence. It’s often the start of getting it back. I’ve seen people come in worried they’ll be limited for good, only to realize that the rehab process is more structured and more manageable than they expected once they understand what each stage is trying to accomplish.
What works: A clear plan, consistent movement, and guidance that matches your surgery and your daily life.
What doesn’t work is treating every patient the same. A retired walker in Scituate, a commuter in Quincy, and someone chasing grandchildren around Weymouth won’t all need the same pacing, same home setup, or same return goals. Good hip surgery rehab has to feel local and personal.
That’s especially true on the South Shore, where daily life includes stairs, uneven sidewalks, beach lots, long drives, and active weekends. Recovery isn’t just about getting from the couch to the kitchen. It’s about getting back to your version of normal with fewer compensations, less fear, and better trust in the new joint.
Preparing for Success Your Pre-Hab Plan in Braintree and Beyond
The smartest part of hip surgery rehab often happens before surgery.
If your body goes into surgery stiff, deconditioned, and unsure how to use the muscles around the hip, your recovery usually feels harder. If you go in stronger and more organized, you’ve given yourself a better starting line. Think of it the way South Shore homeowners think about a Nor’easter. The stronger the setup before the storm, the faster the cleanup after it.
Why doing work before surgery pays off
Evidence for pre-hab is strong. 8-week pre-operative programs have been shown to improve post-op pain, stiffness, hip flexion range of motion, and strength, and fitter patients recover faster after surgery, based on this review of rehabilitation following total hip replacement.
That doesn’t mean you need to train like an athlete. It means your body benefits when you show up to surgery with better baseline strength, better balance, and a clearer understanding of how to move. Patients who’ve done pre-hab also tend to feel less rattled by the first few weeks after surgery because the exercises, the language, and the expectations aren’t brand new.
A useful pre-hab plan usually targets a few key areas:
- Hip and glute strength: especially the muscles that control pelvic stability when you stand on one leg or walk.
- Gentle mobility: enough to keep nearby joints moving well without stirring up more pain.
- Balance and gait: so you’re not learning every movement pattern from scratch after surgery.
- Home planning: walker routes, chair height, stairs, and the setup for sleeping, dressing, and bathing.
Most people don’t need harder exercises before surgery. They need the right ones, done consistently.
What pre-hab looks like in real life
In practical terms, pre-hab often includes sit-to-stands, glute activation, supported balance drills, gentle range-of-motion work, and walking practice with cueing. If pain has made you limp for months, relearning a cleaner pattern ahead of time matters.
It’s also a good phase to sort out what you’ll do at home. Which entrance has fewer steps? Where will the walker fit? Is the bed too low? Can you reach the bathroom safely at night? Those details can reduce stress fast.
Some patients also like using a structured fitness resource outside the clinic to stay consistent with general activity. If that helps you stick with the plan, fully customized workouts can be one way to build routine around the work your therapist gives you.
At this stage, the goal isn’t to chase soreness or prove toughness. The goal is to make the body more prepared and the recovery less chaotic.
The First Weeks Navigating Early Recovery at Home
Coming home after surgery is often the point where everything feels real. The hospital is behind you. The help is more limited. Suddenly small tasks matter a lot, like getting on and off the toilet, stepping into the kitchen, or turning over in bed without holding your breath.
Those first weeks should feel calm and deliberate. Not dramatic. Not heroic. Patients usually do better when they stop trying to “push through” and start treating the early phase like protected healing with purposeful movement.

Set up your home before it becomes a problem
A typical South Shore home can be tricky right after surgery. Split-level layouts, narrow bathrooms, throw rugs, and a few unavoidable steps are common. Make the space boring and predictable.
Use this short checklist:
- Clear the walkway: move rugs, cords, pet bowls, and baskets so your walker or crutches have a straight path.
- Create one main living zone: keep water, medications, chargers, and a phone within easy reach.
- Use the safest chair: choose one with arms and a height that lets you stand without dropping too low.
- Plan for nighttime trips: good lighting matters more than people think, especially when you’re groggy.
If your surgeon gave specific precautions, follow those exactly. The “why” matters. Those restrictions aren’t random. They protect healing tissue and reduce stress on the new joint while the body settles.
What your body needs in the first stretch
Early rehab works best when patients stay active within the plan rather than staying still out of fear. Research shows that within six weeks, patients report a 63% reduction in pain, with meaningful gains in function as summarized in this review of post-operative rehabilitation after hip replacement. That early window matters because it sets the tone for long-term recovery.
The basics are simple:
- Manage swelling and discomfort. Use the pain-control plan your medical team gave you. Ice and elevation are often part of that routine.
- Walk often, not endlessly. Short, frequent walks usually go better than one long session that leaves you swollen and sore.
- Do the assigned exercises. Early movements may feel small, but they help circulation, joint motion, and muscle reactivation.
- Respect the device. If you need a walker or cane, use it. Most setbacks happen when patients ditch support before their body is ready.
If pain rises a little during activity and settles afterward, that’s often workable. If it ramps up and stays elevated, your dose was probably too high.
Families can help by making the environment easier, not by doing every movement for you. Independence returns faster when you stay involved in the process.
For a broader look at what that progression can look like after joint procedures, this Peak article on how post-operative rehabilitation restores mobility after joint surgery is a helpful next read.
Your Rehab Roadmap The Phases of Physical Therapy at Peak
Once you’re cleared for outpatient care, the work gets more specific. Hip surgery rehab transitions from being about getting through the day to restoring a dependable walking pattern, rebuilding strength, and returning to the movements that matter in your life.
The process should feel progressive, but not rushed. A good plan moves forward when your body shows it’s ready, not because the calendar says it should.
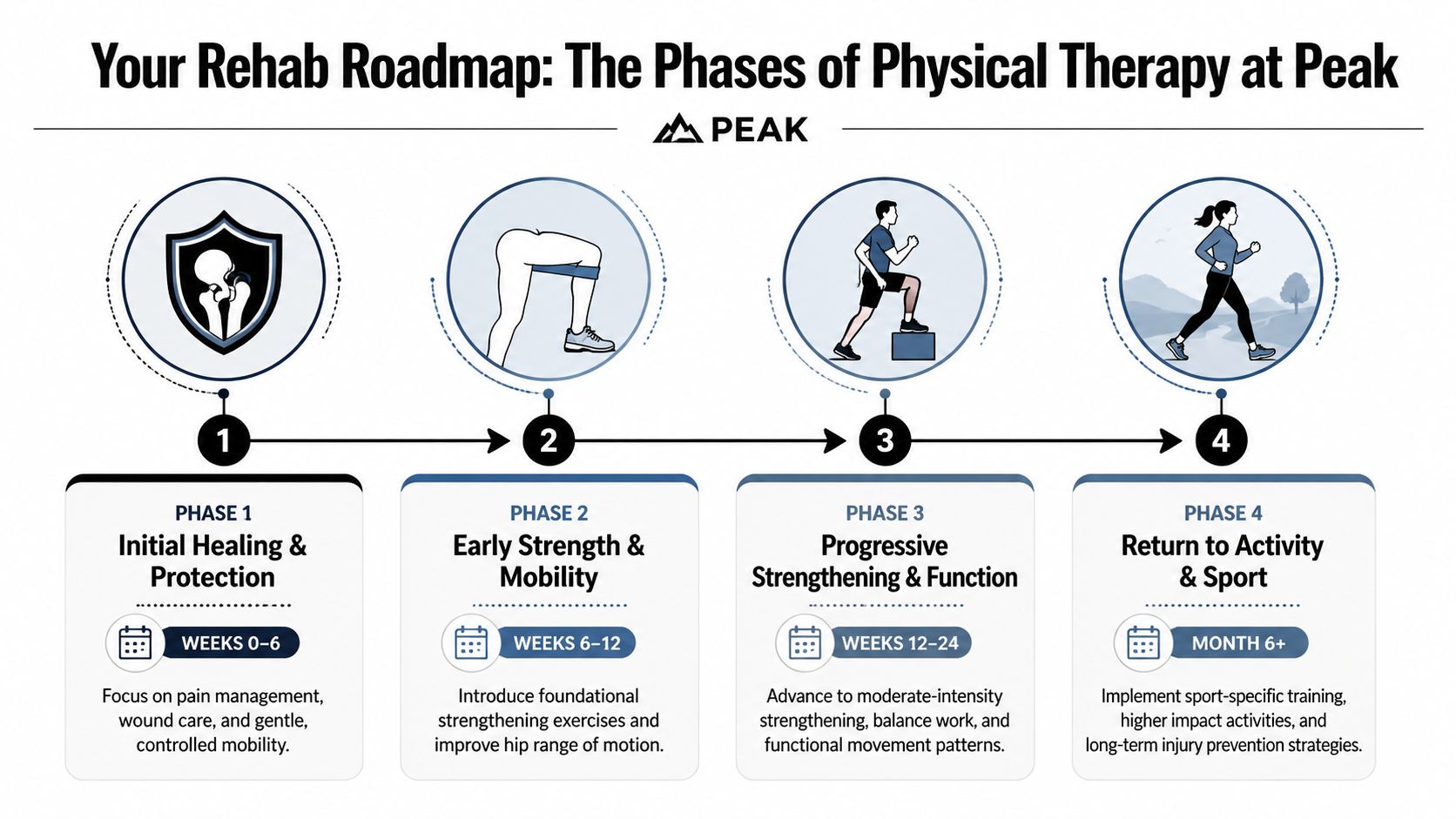
Phase one protect and restore movement
The earliest outpatient phase is about cleaning up the basics. Swelling is still in play. Muscles around the hip may be inhibited. Many patients are still figuring out how to shift weight without bracing.
The focus here is usually:
- Pain and swelling control
- Gentle range of motion within precautions
- Basic muscle activation
- Safe transfers and walking mechanics
Exercises often include isometrics, gentle weight shifts, supported standing work, and simple gait training. This phase can feel almost too easy to motivated patients, but easy is often correct. If you skip quality and go straight to intensity, compensation takes over.
Phase two build control and a normal walking pattern
This is the phase where many people start to feel more like themselves, but it’s also where bad habits can sneak in. Limping, trunk lean, and underusing the surgical side are common if nobody corrects them.
Progression is criterion-based. To move from early to mid-stage rehab, a patient typically needs minimal pain, a normal gait for household distances, and the ability to hold a single-leg stance for more than 20 seconds without hip drop, according to this total hip arthroplasty rehabilitation protocol.
That tells you something important. Advancement isn’t earned by gritting your teeth. It’s earned by control.
A typical middle phase may include:
| Focus area | What it looks like |
|---|---|
| Walking quality | Reducing limp, improving push-off, normalizing step length |
| Foundational strength | Mini-squats, bridges, closed-chain work, hip stability drills |
| Balance | Single-leg control, proprioception, stable pelvic positioning |
| Daily function | Stairs, sit-to-stand, getting in and out of the car |
Patients often ask when exercises “get harder.” The better question is whether the movement looks clean. A shaky single-leg stance tells us more than an extra ten pounds on a machine.
Phase three and beyond rebuild real strength
Later-stage rehab should look more like life. If your goal is to walk the beach in Cohasset, carry groceries up steps in Quincy, or return to golf, your training should eventually reflect those demands. The program becomes more functional, more dynamic, and more specific.
That might include step-downs, loaded sit-to-stands, directional balance work, resisted walking, split-stance strength, and eventually recreational drills if your surgeon clears them. For active adults, this is the phase where confidence catches up to healing.
Clinical reality: Pain can improve before strength, and strength can improve before trust. Good rehab addresses all three.
Late-stage work is also where people realize the value of movement quality. You can finish formal rehab with less pain and still have an avoidable hitch in your gait or weakness during stairs. That’s why home exercise follow-through matters.
If you want examples of movement patterns that often support hip comfort and function, Peak’s guide to hip pain relief exercises is a useful companion.
Not All Hip Surgeries Are the Same How Your Rehab Changes
One of the biggest reasons patients get mixed messages after surgery is simple. Not every hip replacement is approached the same way, so rehab shouldn’t be delivered the same way either.
Generic online advice often falls apart. A patient with a posterior approach may hear “don’t bend past 90 degrees,” while someone with an anterior approach is warned about different motions and may need to delay straight leg raises for 4 to 6 weeks. Those differences are real. They reflect what tissues were disturbed during surgery and what positions stress the healing area.
Posterior approach rehab
Posterior approach patients usually need to be more careful with positions that combine hip flexion, adduction, and internal rotation. That caution exists because the back of the hip has to heal, and the dislocation risk is higher if precautions are ignored. Reported posterior dislocation risk reaches 3.23%, according to this discussion of approach-specific rehab differences after hip replacement.
In practical terms, early rehab for a posterior approach often means more attention to sitting height, how you pivot, how you get in and out of a car, and how you turn in bed. Therapists also watch walking mechanics closely because patients may guard the hip and overuse the trunk.
Anterior approach rehab
Anterior approach patients are often told a different set of restrictions. They may not have the same classic posterior precautions, but that doesn’t mean they can do everything immediately. One common issue is moving too aggressively too soon because the front-side approach can feel easier in the early days.
Straight leg raises may be delayed for 4 to 6 weeks with anterior cases, and extension-based positions may be monitored more carefully depending on the surgeon’s instructions. The body still needs protection while irritated tissues settle and strength returns.
Why this matters to patients on the South Shore
This is exactly why local follow-up matters. If you were told one thing by a friend in Plymouth and something different by your surgeon in Boston, both could be correct for different operations.
The safest question isn’t “What do people do after hip replacement?” It’s “What does my specific surgery require, and how does that affect my walking, stairs, car transfers, and exercise progression?” That’s the kind of detail patients deserve.
For a local overview tied more directly to recovery after this procedure, Peak’s article on physical therapy after hip replacement is a practical place to keep reading. For broader educational content about anatomy and recovery concepts, Highbar Health’s resource library at highbarhealth.com is the better hub.
Getting Back to Your Life Timelines for Driving Sports and Work
Most patients don’t ask me whether they’ll ever do a clamshell again. They ask when they can drive, work, sleep on their side, walk the dog, or get back to nine holes without paying for it the next day.
Those are the right questions. The challenge is that return-to-activity timelines aren’t one-size-fits-all. They depend on pain control, medication use, side of surgery, gait quality, strength, balance, surgical approach, and what you’re trying to return to.

The milestone that matters most
A lot of people think “full recovery” means no pain. In reality, late-stage success is more demanding than that. Many patients do well long term, but 70% to 80% achieve good outcomes while 20% to 30% can still have persistent hip rotation deficits, based on this discussion of longer-term hip rehab expectations and late-stage function. That’s why advanced rehab often focuses on sport-specific work and getting to more than 90% strength symmetry before higher-demand return.
That has real-life implications on the South Shore. If you want to carry beach chairs through sand, rotate through a golf swing, or handle long walks at Wompatuck without shifting everything into your back, rotation and side-to-side strength matter.
Better pain relief doesn’t automatically mean better performance. Late-stage capacity has to be built.
What return to activity usually depends on
Here’s the practical way to think about common milestones:
- Driving: You need to move the leg confidently, get in and out of the car safely, and be off any medication that would make driving unsafe. This is a safety decision, not just a time decision.
- Desk work: Some people return earlier if they can sit comfortably, stand often, and manage transportation. Others need longer if commuting or sitting tolerance is still limited.
- Physical jobs: These usually require a more complete strength and movement recovery because lifting, carrying, climbing, and prolonged standing expose weakness quickly.
- Walking for exercise: This often returns before recreational sport, but distance should build gradually.
- Golf, pickleball, and more active recreation: These require rotational control, balance, and confidence. They’re not just “walking plus.”
For older adults who need extra help at home during this stretch, especially with transportation or daily routines, it can be reassuring to know that personalised home care can support independent living while therapy handles the rehab side.
A good return plan isn’t based on optimism alone. It’s based on whether your hip can absorb the demand without swelling, limping, or forcing compensation into your back and opposite leg.
Your Local Partner Peak PT in Quincy Plymouth and Across the South Shore
When you’re ready to start, convenience matters more than people expect. Rehab is rarely one visit. You need a clinic location that fits your week and a process that doesn’t add more friction while you’re already managing appointments, paperwork, and recovery logistics.
Peak serves communities across the South Shore, including Braintree, Quincy, Weymouth, Cohasset, Duxbury, East Bridgewater, Hanover, Kingston, Milton, Norwell, Pembroke, Plymouth, and Scituate. That makes it easier to schedule around work, family responsibilities, and the realities of getting around after surgery.
Where to get started
The first step is simple. Book an evaluation at the clinic that’s easiest for you to reach. If you’ve already had surgery, bring the post-op instructions and any precautions from your surgeon. If surgery is coming up, ask for a pre-hab visit so the plan starts before the procedure.
Peak Physical Therapy and Sports Performance provides post-surgical rehabilitation, guided exercise, and hands-on care for orthopedic recovery across these South Shore locations.
What to bring to your first visit
A smooth first appointment usually starts with the basics:
- Your referral or prescription, if one was provided
- Insurance information
- Your surgeon’s protocol or discharge paperwork
- A list of questions about stairs, driving, work, or activity goals
- Supportive clothing and shoes you can move in
Good rehab should feel organized from day one. You should know what the first goals are, what to do at home, what to avoid, and what signs mean you need to check in sooner.
If you want a deeper educational library on orthopedic recovery topics beyond this local guide, visit highbarhealth.com.
Frequently Asked Questions About Hip Rehab
How long will I need a walker or cane
Long enough to walk without a limp. That answer matters more than any fixed timeline. If you stop using a device before your hip can control your body weight, you usually trade the walker for a compensation pattern.
What are red flags during recovery
Call your surgeon or medical team if you notice unexpected changes that feel clearly outside your normal recovery pattern, especially worsening symptoms, unusual wound concerns, or a sudden drop in function. If something feels off, don’t wait and guess.
Recovery should feel gradually demanding, not suddenly alarming.
How often will I go to physical therapy
That depends on the stage of recovery, your surgical precautions, your home support, and how independently you can perform the plan. Some people need closer supervision early. Others progress well with fewer visits and strong follow-through at home.
What if pain increases after a session
A mild temporary increase can happen when activity expands. Pain that remains high, comes with more swelling, or changes how you walk usually means the exercise dose was too high or the movement quality wasn’t there yet. Tell your therapist so the plan can be adjusted instead of abandoned.
What makes a good hip surgery rehab plan
Three things. It should match your surgical approach, use clear progression criteria, and connect rehab to your actual life. If your goal is stairs, dog walking, gardening, golf, or beach walking, the plan should prepare you for those tasks instead of stopping at basic exercises.
If you’re dealing with hip pain now or getting ready for surgery, the next step is to put a clear local plan in place. Peak Physical Therapy and Sports Performance helps South Shore patients move from pre-hab to post-op recovery with practical guidance, individualized treatment, and convenient clinic access across the region. Book an appointment and get answers that fit your surgery, your home, and the life you want to return to.